Volume 6, Number 4—August 2000
Dispatch
The Role of Pathology in an Investigation of an Outbreak of West Nile Encephalitis in New York, 1999
Abstract
An outbreak of encephalitis occurred in New York City in late August 1999, the first caused by West Nile virus in North America. Histopathologic and immunopathologic examinations performed on human autopsy materials helped guide subsequent laboratory and epidemiologic investigations that led to identification of the etiologic agent.
In August 1999, the New York City Department of Health identified a cluster of eight patients with encephalitis, seven of whom had profound muscle weakness (1,2). These cases were initially thought to have been caused by St. Louis encephalitis (SLE) virus, a member of the genus Flavivirus, family Flaviviridae, on the basis of temporal, geographic, and epidemiologic similarities in the cases, clinical histories, identification of flaviviral immunoglobulin M (IgM) and IgG antibodies in serum and cerebrospinal fluid from suspected patients, and positive immunohistochemical staining for flaviviral antigens in tissue sections from the central nervous system of fatal cases.
Despite this early evidence, doubts remained as to whether SLE virus was the etiologic agent. Polymerase chain reaction (PCR) test results were negative when SLE virus-specific primers were used, and subsequent serologic testing using virus-specific plaque-reduction neutralization tests for SLE virus revealed only low-level SLE virus-neutralizing antibodies. Increased fatalities among crows and other birds, a phenomenon usually not associated with an SLE outbreak, were also being concurrently reported. Since the antibody used in immunohistochemical tests was known to cross-react with several members of the Japanese encephalitis virus serocomplex (which includes Japanese encephalitis virus, SLE virus, and West Nile virus) the initial serologic and immunohistochemical results could not exclude the possibility of another related flavivirus as the cause of the outbreak. Moreover, immunohistochemical testing of tissue from four fatal human cases indicated a high concentration of flavivirus in the brain stem and spinal cord. Subsequent reverse transcriptase-PCR tests, using several degenerate primer sets designed to detect conserved regions within a wide variety of flaviviruses, together with West Nile virus-specific primer sets, identified West Nile virus as the etiologic agent of both the human outbreak and the equine and avian epizootics (3-5). This was the first reported outbreak of encephalitis caused by West Nile virus in North America.
Figure 1
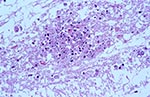
Figure 1. Neuronal necrosis with infiltrates of microglia and polymorphonuclear leukocytes. Hematoxylin-eosin staining. Original magnification, X100.
Figure 2
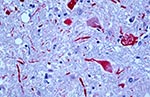
Figure 2. Positive staining of viral antigens in neurons and neuronal processes. Immunoalkaline phosphate staining, naphthol fast red substrate with light hematoxylin counterstain. Original magnification, X100.
Histopathologic examination of four fatal human cases showed varying degrees of neuronal necrosis in the gray matter, with infiltrates of microglia and polymorphonuclear leukocytes, perivascular cuffing, neuronal degeneration, and neuronophagia (Figure 1). Immunohistochemical staining demonstrated viral antigens in neurons, neuronal processes, and areas of necrosis (Figure 2). No immunostaining was seen in other major organs, including lung, liver, spleen, and kidney. The histopathologic lesions and immunostaining were more prominent in the brain stem and spinal cord, which may explain the clinical manifestation of muscle weakness in some patients.
These pathologic studies were critical to the eventual discovery of West Nile virus for several reasons. First, the initial examination of human autopsy specimens suggested a correlation between the histopathologic features of fatal cases and cases with serologic and immunohistochemical evidence of flavivirus infection. This correlation gave researchers increased confidence in the diagnosis in the early stage of the investigation. Second, infections of the central nervous system have important clinical significance because they can cause neurologic damage and death. Clinical manifestations, epidemiologic information, and patient history--while frequently suggestive of a diagnosis--are often unreliable for determining the specific cause of a central nervous system infection. A specific etiologic diagnosis is particularly important in this era of ever-changing environmental and ecological factors and increased awareness of atypical disease presentations. Localization of West Nile virus antigens by immunohistochemical analysis, in conjunction with classic histopathologic examination, is a prime example of how new pathologic techniques are being used in investigations of outbreaks caused by emerging infections (6). Third, the topographic distribution of histopathologic lesions and flaviviral antigens in the brain stem and spinal cord guide subsequent PCR testing. Such information also helps explain the clinical manifestations of illness and suggests that virus spread through neuronal processes plays an important role in the pathogenesis of human West Nile virus infection.
Autopsy rates are decreasing in the United States and worldwide (7). This decline has been influenced by escalating costs, jurisdictional and authorization uncertainties, and undue emphasis on antemortem diagnostic technologies. In this outbreak, autopsies were performed under the jurisdiction of New York City's Office of Chief Medical Examiner because of the obvious public health implications (8). Other notable recent examples in which autopsy contributed to the discovery or better understanding of emerging infectious diseases include investigations of hantavirus pulmonary syndrome, Ebola hemorrhagic fever, leptospirosis associated with pulmonary hemorrhage, new variant Creutzfeldt-Jakob disease, and Nipah virus encephalitis (9). These examples underscore the need to increase autopsy rates to detect infectious diseases (10,11).
Although it is not known when and how West Nile virus was introduced into North America, possible mechanisms include international travel of infected persons to New York City or transport of virus by mosquitoes, ticks, or imported infected birds. Many factors are associated with the geographic spread and emergence and distribution of zoonotic pathogens, including demographic and societal changes, modern methods of transportation, changing geoclimatic conditions, migration of animals and birds, and alteration of arthropod reservoirs and vectors. Collaboration among scientists from diverse fields--such as epidemiology, clinical and veterinary medicine, entomology, microbiology, and pathology--will advance the recognition of emerging zoonotic infections (9,11,12). The investigation of this outbreak of West Nile encephalitis demonstrates the value of such a multidisciplinary approach.
Dr. Shieh is a staff pathologist, Infectious Disease Pathology Activity, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases, Centers for Disease Control and Prevention. His research interests include infectious disease pathology; pathology and pathogenesis of viral encephalitides; and infectious disease outbreak investigations.
References
- Centers for Disease Control and Prevention. Outbreak of West Nile-like viral encephalitis--New York, 1999. MMWR Morb Mortal Wkly Rep. 1999;48:845–9.PubMedGoogle Scholar
- Asnis DS, Conetta R, Teixeira AA, Waldman G, Sampson BA. The West Nile virus outbreak of 1999 in New York: the Flushing Hospital experience. Clin Infect Dis. 2000;30:413–8. DOIPubMedGoogle Scholar
- Lanciotti RS, Roehrig JT, Deubel V, Smith J, Parker M, Steele K, Origin of the West Nile virus responsible for an outbreak of encephalitis in the northeastern United States. Science. 1999;286:2333–7. DOIPubMedGoogle Scholar
- Briese T, Jia XY, Huang C, Grady LJ, Lipkin WI. Identification of a Kunjin/West Nile-like flavivirus in brains of patients with New York encephalitis. Lancet. 1999;354:1261–2. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Update: West Nile-like viral encephalitis--New York, 1999. MMWR Morb Mortal Wkly Rep. 1999;48:944–6, 955.
- Shieh W-J, Guarner J, Greer P, Morken T, Bartlett J, Ferebee T, Histopathologic and immunohistochemical studies for acute viral encephalomyelitis in formalin-fixed human tissues. Lab Invest. 1999;79:153A.
- Hanzlick R, Baker P. Case of the month: institutional autopsy rates. Arch Intern Med. 1998;158:1171–2. DOIPubMedGoogle Scholar
- Sampson BA, Ambrosi C, Charlot A, Reiber K, Veress JF, Armbrustmacher V. The pathology of human West Nile virus infection. Hum Pathol. 2000;31:527–31. DOIPubMedGoogle Scholar
- Zaki SR, Paddock CD. The emerging role of pathology in infectious diseases. Emerging Infections 3. In: Scheld WM, Craig WA, Hughes JM, editors. Washington: American Society for Microbiology Press; 1999. p.181-200.
- Schwartz DA. Emerging and reemerging infections. Progress and challenges in the subspecialty of infectious disease pathology. Arch Pathol Lab Med. 1997;121:776–84.PubMedGoogle Scholar
- Nolte KB, Simpson GL, Parrish RG. Emerging infectious agents and the forensic pathologist: the New Mexico model. Arch Pathol Lab Med. 1996;120:125–8.PubMedGoogle Scholar
- Brown C. Emerging diseases--what veterinarians need to know. J Vet Diagn Invest. 1997;9:113–7.PubMedGoogle Scholar
Figures
Cite This ArticleTable of Contents – Volume 6, Number 4—August 2000
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Sherif Zaki, National Center for Infectious Diseases, Centers for Disease Control and Prevention, 1600 Clifton Rd, Mail Stop G32, Atlanta, GA 30333, USA; fax: 404-639-3043
Top