Volume 14, Number 10—October 2008
Dispatch
Unexplained Deaths and Critical Illnesses of Suspected Infectious Cause, Taiwan, 2000–2005
Figure
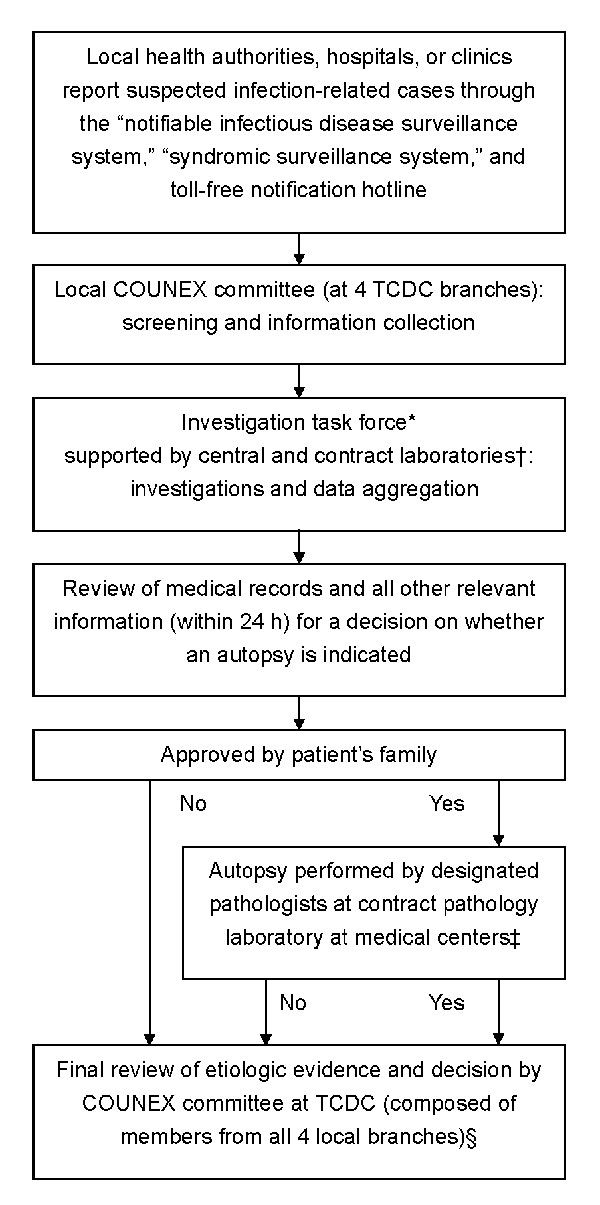
Figure. Flow of information and decision making for reported cases of unexplained death or critical illness. *If unexplained infectious causes were suspected, COUNEX mobilized an investigation team including experts, field epidemiology training program members, public health workers from the local branch of Taiwan Centers for Disease Control (TCDC), and public health authorities to proceed with further field investigation. TCDC was in charge of the investigation. †Cases were categorized into >1 of the following clinical syndromes: acute neurologic (encephalitis, meningitis), acute respiratory (pneumonia), acute hemorrhagic, acute diarrhea, acute jaundice (hepatitis), acute heart (myocarditis, pericarditis, endocarditis), and acute kidney-related. For every reported case, COUNEX investigators usually selected diagnostic tests relevant to a particular syndrome (www.cdc.gov.tw). Additional tests were prescribed if needed. The hospital laboratories were requested to save all remaining clinical specimens, including biopsy specimens, obtained from clinical management and send them to our reference laboratories, if indicated. ‡If an autopsy was performed, whenever possible tissue specimens were examined by pathologists of TCDC-designated medical centers and the Forensic Department of the Ministry of Justice to ensure the accuracy of the final diagnosis. Specimens were also sent for microbiologic cultures and tests as well as toxicologic examination for trace toxic chemicals, if needed. §All laboratory results and clinical, epidemiologic, and pathologic data were sent to the expert committee to determine if the etiologic agent could fully or most likely explain the disease. Otherwise, cases were categorized as unexplained. In general, histopathogic examination was the major evidence for determining cause. If case-patients could not be autopsied within 36 hours of death, laboratory results would be the most useful information for identification of cause of death.