Volume 13, Number 3—March 2007
Letter
Amebic Liver Abscess in HIV-infected Patients, Republic of Korea
Cite This Article
Citation for Media
To the Editor: Amebic liver abscess (ALA) is the most common extraintestinal complication of amebic infection. Although loss of cellular immunity is thought to play a role in infection by the pathogen, whether HIV infection is also a risk factor for invasive amebiasis is controversial (1–3). ALA in HIV-infected patients has not been well characterized, although several case series have been reported (2,4). We report the role of HIV infection status in ALA in an area where ALA is not endemic and the clinical features of ALA in HIV-infected patients.
All patients with ALA at Seoul National University Hospital (SNUH) from January 1990 through December 2005 were identified; some have been previously reported (5). SNUH is a 1,600-bed, university-affiliated teaching hospital and the largest referral center for HIV/AIDS in the Republic of Korea. The diagnostic criteria for ALA were radiologic evidence of intrahepatic abscess, trophozoites of Entamoeba histolytica in fluid aspirated from an abscess, or absence of bacteria and fungi in aspirated fluid and a titer ≥128 in an indirect hemagglutination assay (IHA) for E. histolytica.
Figure
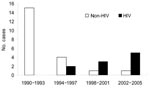
Figure. Number of cases of amebic liver abscess in patients with and without HIV infection at Seoul National University Hospital, Republic of Korea, 1990–2005.
Of 31 patients with ALA at SNUH from 1990 through 2005, 10 (32%) were HIV positive. The proportion of HIV-infected patients among patients with ALA increased significantly with time (linear-by-linear association, p<0.001) (Figure). Of 10 patients from 1998 through 2005, 8 (80%) were HIV positive. Except for 2 patients with a history of travel to an ALA-endemic area, 88% of the patients were HIV positive.
Median age of the 10 HIV-positive patients with ALA was 34.5 years (range 29–54 years); all patients were male. Four had a homosexual orientation, 4 had a heterosexual orientation, and 2 had an unknown sexual orientation. Fever (100%) was the most common symptom, and abdominal tenderness (90%) and diarrhea (50%) were frequently observed. Median leukocyte count was 9,000/mm3 (range 3,410–16,700/mm3), and median CD4 cell count was 279/mm3 (range 40–370/mm3). Eight patients had abscesses in the right lobe of the liver and 2 had abscesses in both lobes; 8 patients had 1 abscess and 2 had multiple abscesses. Median size of abscesses was 7.25 cm (range 3–12 cm). In 5 patients, pleural effusion was observed in chest radiographs. IHA titer was ≥128 in 10 patients and ≥512 in 8 patients. Median days to defervescence was 2 (range 1–5 days). In 2 patients, perforation of the abscess into the abdominal cavity was a complication. No patients died or had relapses.
Early in the AIDS pandemic, some studies reported that the prevalence of invasive amebiasis was not increased in patients with HIV infection (1,6). However, recent reports of ALA associated with HIV infection have increased. Studies in Taiwan demonstrated that invasive amebiasis, including ALA, is on the increase in HIV-infected patients in disease- endemic areas (2,7).
Amebiasis was previously an endemic disease in the Republic of Korea. The positive rate for cysts of E. histolytica/E. dispar in the general population was 10% in the 1960s (5). However, with improvements in sanitation, this rate decreased to 0.5% in 1993 and to nearly 0% in 2004 (8). The present study showed that ALA in association with HIV infection is increasing in the Republic of Korea, and that ALA in HIV-negative patients has greatly decreased. In a study in the United States, 38% of patients with ALA with no history of travel to a disease-endemic area were HIV positive (3). These results support the view that ALA is an emerging parasite infection in HIV-infected patients in non–disease-endemic areas, as well as in disease-endemic areas.
Immune suppression is an important risk factor for ALA. In animal studies, immune suppression after thymectomy or splenectomy results in an increased incidence of ALA (9). Suppressed cellular immunity caused by use of steroids and malnourishment predispose to fatal amebiasis (10). In the present study, 90% of patients had CD4 cell counts <350/mm3, which implies that immune suppression by HIV infection may be another risk factor for ALA.
Only 2 patients with pyogenic liver abscess were observed during the study. In these patients, pyogenic liver abscess was diagnosed, despite negative cultures for bacteria and fungi, because trophozoites of E. histolytica were not demonstrated in aspirated pus, and results of IHA for amebiasis were negative. However, we cannot exclude amebic liver abscess in these 2 patients because IHA test results can be negative in HIV-infected patients (2).
This study suggests that ALA is an emerging parasite infection in HIV-infected patients even in areas where the disease is not endemic. ALA should be considered in HIV-infected patients with space-occupying lesions in the liver, and HIV screening is strongly recommended in patients in areas where ALA is not endemic, especially those with no history of travel to a disease-endemic area.
References
- Jessurun J, Barron-Rodriguez LP, Fernandez-Tinoco G, Hernandez-Avila M. The prevalence of invasive amebiasis is not increased in patients with AIDS.AIDS. 1992;6:307–9. DOIPubMedGoogle Scholar
- Hung CC, Chen PJ, Hsieh SM, Wong JM, Fang CT, Chang SC, Invasive amoebiasis: an emerging parasitic disease in patients infected with HIV in an area endemic for amoebic infection.AIDS. 1999;13:2421–8. DOIPubMedGoogle Scholar
- Seeto RK, Rockey DC. Amebic liver abscess: epidemiology, clinical features, and outcome.West J Med. 1999;170:104–9.PubMedGoogle Scholar
- Wiwanitkit V. A note on clinical presentations of amebic liver abscess: an overview from 62 Thai patients.BMC Fam Pract. 2002;3:13. DOIPubMedGoogle Scholar
- Oh MD, Lee K, Kim E, Lee S, Kim N, Choi H, Amoebic liver abscess in HIV-infected patients.AIDS. 2000;14:1872–3. DOIPubMedGoogle Scholar
- Reed SL, Wessel DW, Davis CE. Entamoeba histolytica infection and AIDS.Am J Med. 1991;90:269–71.PubMedGoogle Scholar
- Liu CJ, Hung CC, Chen MY, Lai YP, Chen PJ, Huang SH, Amebic liver abscess and human immunodeficiency virus infection: a report of three cases.J Clin Gastroenterol. 2001;33:64–8. DOIPubMedGoogle Scholar
- Chai JY, Park JH, Guk SM, Kim HJ, Kim JL, Gu YS, Status of intestinal parasite infections among 4,137 residents from provinces nationwide and metropolitan areas in the Republic of Korea (2004). Journal of Infection and Chemotherapy.2006;38:198–203.
- Ghadirian E, Meerovitch E. Effect of immunosuppression on the size and metastasis of amoebic liver abscesses in hamsters.Parasite Immunol. 1981;3:329–38. DOIPubMedGoogle Scholar
- Eisert J, Hannibal JE, Sanders SL. Fatal amebiasis complicating corticosteroid management of pemphigus vulgaris.N Engl J Med. 1959;261:843–5.PubMedGoogle Scholar
Figure
Cite This ArticleRelated Links
Table of Contents – Volume 13, Number 3—March 2007
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Kang Won Choe, Department of Internal Medicine, Seoul National University College of Medicine, 28 Yeongun-dong, Chongro-gu, Seoul, Republic of Korea, 110-744; Kang Won Choe, Department of Internal Medicine, Seoul National University College of Medicine, 28 Yeongun-dong, Chongro-gu, Seoul, Republic of Korea, 110-744;
Top