Volume 16, Number 1—January 2010
Letter
Otomastoiditis Caused by Mycobacterium abscessus, the Netherlands
Cite This Article
Citation for Media
To the Editor: Nontuberculous mycobacteria (NTM) are increasingly recognized as human pathogens (1). Otomastoiditis is a rare extrapulmonary NTM disease type first described in 1976; Mycobacterium chelonae–M. abscessus group bacteria, which are rapidly growing NTM, are the most frequent causative agents and the disease mostly affects children (1–3). In the Netherlands, M. chelonae–M. abscessus group isolates have been reported from the otologic samples of an average of 2 patients annually since 2006, as compared to 6 patients in the preceding 10 years. This emergence is not a likely result of improved laboratory facilities or awareness in clinicians because liquid culture and molecular identification techniques predate the rise in notification and Dutch guidelines advise against performing cultures for chronic otorrhea.
We identified 10 patients from the national reference laboratory database with otologic samples yielding M. chelonae–M. abscessus group bacteria during January 1995–June 2007. We resubjected these isolates to molecular identification by rpoB gene sequencing (4) and performed a medical file review.
The rpoB gene sequencing showed that M. abscessus was the causative agent in all 10 cases; M. abscessus seems to have a predilection to cause otomastoiditis. Closely related M. bolletii and M. massiliense (4) were not found. Early reports identified M. fortuitum or M. chelonae as causative agents, which may be because the taxonomy of the rapidly growing NTM has long been debated (2,4–7); many of these agents may have, in fact, been M. abscessus. All primary isolates were found susceptible to clarithromycin and resistant to fluoroquinolones and aminoglycosides in our agar dilution method (8), which is not the recommended method for rapidly growing NTM (1). Two patients acquired clarithromycin resistance during treatment.
Clinical data are summarized in the Appendix Table and match those of previous studies (3,5,6). All patients had a history of ear infections and tympanostomy tube placement, previously associated with NTM disease (7). Nine patients had used ototopical medication, including quinolone antimicrobial agents (n = 5), steroids, aminoglycosides (n = 2), or both (n = 2). Clinical signs were nonspecific, with persistent tympanic membrane perforation, chronic painless otorrhea resistant to antimicrobial drug therapy, and hearing loss.
The fact that this disease primarily affects children, with a mean age of 6 years, may be related to age-specific environmental exposures, e.g., playing in sand pits or swimming (9). Two patients with M. abscessus otomastoiditis are siblings (patients 5 and 6); a clonal relationship between the causative bacteria is possible and should be investigated by molecular typing tools.
Appendix Figure
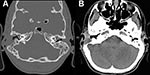
Appendix Figure. Computed tomography images of a patient with Mycobacterium abscessus otomastoiditis. Extensive bone destruction in the right mastoid and associated right-sided mucosal swelling can be seen. A) Bone tissue window setting; B)...
Primary isolates were from biopsy material (n = 5) or otorrhea fluid (n = 5) and were positive for acid-fast bacilli by direct microscopy for 9 patients. Five patients had a computed tomography (CT) scan performed, which showed fluid in the mastoid (n = 4), bone erosion of the mastoid (n = 2), and mucosal swelling (all); the Appendix Figure displays typical findings.
The mean interval between first symptoms and diagnosis of M. abscessus otomastoiditis was 155 days for (range 14–360 days). Otorrhea unresponsive to antimicrobial drug therapy should raise a clinical suspicion of NTM otomastoiditis (3), especially in patients with bone destruction visible on CT images. In patients with otorrhea unresponsive to antimicrobial drug therapy, routine CT scanning and Mycobacterium spp. cultures, preferably from tissue biopsies (1), may reduce diagnostic delay and prevent further damage.
Patients with M. abscessus otomastoiditis received drug treatment for a mean duration of 3 months (range 28–150 days) and 1.8 episodes of surgery. Five patients with M. abscessus otomastoiditis received clarithromycin monotherapy; 5 received multidrug therapy with fluoroquinolones (n = 3), fluoroquinolones, rifampin, and ethambutol (n = 1), or meropenem (n = 1 (Appendix Table).
Complications of surgery comprised delayed wound healing (n = 4) and fistula formation (n = 2; Appendix Table). Two patients underwent incus removal and later chain reconstruction surgery (patients 7 and 8). In 1 patient, the infection spread and caused culture-proven cervical lymphadenitis, a retroauricular abscess, fistula, and facial nerve palsy.
Eight patients were eventually cured, defined by symptomatic improvement and in some cases confirmed by negative cultures. Two patients were still receiving treatment at the time of data collection. Five patients had persistent conductive hearing loss after treatment (42%; range 30–80 dB; Appendix Table).
American Thoracic Society guidelines for treatment of soft tissue and bone infections caused by M. abscessus advocate 4–6 months of therapy with a macrolide, an aminoglycoside and cefoxitin or a carbapenem, based on in vitro drug susceptibility test results, combined with surgical debridement when possible (1). Treatment regimens in this study deviated in duration and content; clarithromycin monotherapy is likely to invoke resistance (1) and no evidence supports fluoroquinolone use (1). Moreover, use of parenteral agents was limited; its reasoning was not generally captured during file review.
M. abscessus otomastoiditis is a serious, potentially emerging condition that affects children who have had previous infections, tympanostomy tubes, and ototopical antimicrobial drug or steroid use in the Netherlands. The diagnostic delay and treatment regimens warrant improvement to prevent deterioration, additional episodes of surgery, acquired drug resistance, and to prevent or limit permanent hearing loss.
References
- Griffith DE, Aksamit T, Brown-Elliot BA, Catanzaro A, Daley C, Gordin F, An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175:367–416. DOIPubMedGoogle Scholar
- Austin WK, Lockey MW. Mycobacterium fortuitum mastoiditis. Arch Otolaryngol. 1976;102:558–60.PubMedGoogle Scholar
- Franklin DJ, Starke JR, Brady MT, Brown BA, Wallace RJ Jr. Chronic otitis media after tympanostomy tube placement caused by Mycobacterium abscessus: a new clinical entity? Am J Otol. 1994;15:313–20.PubMedGoogle Scholar
- Adékambi T, Berger P, Raoult D, Drancourt M. rpoB gene sequence-based characterization of emerging non-tuberculous mycobacteria with descriptions of Mycobacterium bolletii sp. nov., Mycobacterium phocaicum sp. nov. and Mycobacterium aubagnense sp. nov. Int J Syst Evol Microbiol. 2006;56:133–43. DOIPubMedGoogle Scholar
- Lowry PW, Jarvis WR, Oberle AD, Bland LA, Silberman R, Bocchini JA Jr, Mycobacterium chelonae causing otitis media in an ear-nose-and-throat practice. N Engl J Med. 1988;319:978–82.PubMedGoogle Scholar
- Flint D, Mahadevan M, Gunn R, Brown S. Nontuberculous mycobacterial otomastoiditis in children: four cases and a literature review. Int J Pediatr Otorhinolaryngol. 1999;51:121–7. DOIPubMedGoogle Scholar
- De Groote MA, Huitt G. Infections due to rapidly growing mycobacteria. Clin Infect Dis. 2006;42:1756–63. DOIPubMedGoogle Scholar
- van Klingeren B, Dessens-Kroon M, van der Laan T, Kremer K, van Soolingen D. Drug susceptibility testing of Mycobacterium tuberculosis complex by use of a high-throughput, reproducible, absolute concentration method. J Clin Microbiol. 2007;45:2662–8. DOIPubMedGoogle Scholar
- Lindeboom JA, Prins JM, Bruijnesteijn van Coppenraet ES, Lindeboom R, Kuijper EJ. Cervicofacial lymphadenitis in children caused by Mycobacterium haemophilum. Clin Infect Dis. 2005;41:1569–75. DOIPubMedGoogle Scholar
Figure
Cite This ArticleRelated Links
Table of Contents – Volume 16, Number 1—January 2010
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Jakko van Ingen, RIVM;LIS, National Mycobacteria Reference Laboratory (pb22), PO Box 1, 3720BA Bilthoven, the Netherlands
Top