Volume 22, Number 11—November 2016
Dispatch
Severe Fever with Thrombocytopenia Syndrome Complicated by Co-infection with Spotted Fever Group Rickettsiae, China
Cite This Article
Citation for Media
Abstract
During 2013–2015 in central China, co-infection with spotted fever group rickettsiae was identified in 77 of 823 patients infected with severe fever with thrombocytopenia syndrome virus. Co-infection resulted in delayed recovery and increased risk for death, prompting clinical practices in the region to consider co-infection in patients with severe fever with thrombocytopenia syndrome.
In recent years, new tickborne pathogens have increasingly emerged, creating public health challenges. Co-infection may occur in humans either through the bite of 1 tick co-infected with multiple pathogens or bites of multiple ticks, each carrying a different pathogen (1).
In 2009, severe fever with thrombocytopenia syndrome virus (SFTSV) was identified in humans in China, and since then, the virus has been detected in 19 provinces (2). The most highly affected region is in central China, where over one third of cases have been reported. Another tickborne pathogen, Candidatus Rickettsia tarasevichiae, classified among the spotted fever group rickettsiae (SFGR), was first identified in 2012 in the northeastern area of China, but is now infecting humans in the more densely populated central region (3). SFGRs have been detected in Haemaphysalis longicornis ticks (3,4), which also serve as a competent vector for SFTSV (5). In 2014, Candidatus R. tarasevichiae infection was detected in SFTSV-infected persons in eastern central China, indicating that co-infection with SFGR might be common among SFTSV-infected persons in the region (3). To determine the effects of co-infection with SFGR in SFTSV-infected persons, we compared clinical characteristics and laboratory findings for patients with SFTSV infection only with those for patients co-infected with SFTSV and Candidatus R. tarasevichiae.
During 2013–2015, we conducted a retrospective investigation at the 154 Hospital of the People’s Liberation Army in Xinyang City, Henan Province, China. All patients meeting the criteria for having suspected severe fever with thrombocytopenia syndrome (SFTS) were enrolled (6). Serial serum and anti-coagulated blood samples were collected from patients throughout hospitalization and during convalescence.
RNA detection by reverse transcription PCR and serologic testing by ELISA were performed for diagnosis of SFTSV infection (6). SFTSV infection was determined by the detection of viral RNA in serum, seroconversion, or a 4-fold increase in SFTSV-specific IgG titers in paired serum samples collected >2 weeks apart. We used an indirect immunofluorescence assay (Focus Diagnostic, Cypress, CA, USA) to detect Rickettsia rickettsii IgG. Acute SFGR infection was defined as seroconversion or a 4-fold increase in R. rickettsii IgG titers in paired serum samples. We measured serum levels of cytokines and chemokines by using a Bio-Plex Pro Human Cytokine 27-plex Assay (Bio-Rad, Hercules, CA, USA).
For the study, we recruited 823 SFTS patients who had paired serum samples available for testing (Technical Appendix Table 1). Of those patients, 77 (8.5%) also had serologic evidence of SFGR infection: 45 showed seroconversion, and 32 had a 4-fold increase in IgG titers. Those 77 patients represented the SFTSV–SFGR co-infection group (Technical Appendix Table 2); the other 746 patients represented the SFTSV single-infection group.
Influenza-like symptoms were the most common clinical manifestations in both groups, and, except for fever, which was more prolonged in the co-infection group (p = 0.039), symptoms were comparable in the groups (Technical Appendix Table 3). Ascites and hemorrhagic signs were more common in the co-infection than the single-infection group (p = 0.002 and p = 0.003, respectively). The frequencies of other complications, including gastrointestinal, respiratory, and neurologic syndromes, were similar in the 2 groups.
Figure 1
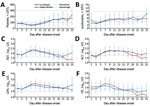
Figure 1. Dynamic profiles for 6 selected laboratory parameters for hospitalized patients with severe fever with thrombocytopenia syndrome virus (SFTSV) infection only or with SFTSV and spotted fever group rickettsiae co-infection, China, 2013–2015....
At hospital admission, the co-infection group had longer prothrombin times (Table). For both groups, thrombocytopenia occurred starting at 4 days after symptom onset and persisted for as long as 2 weeks (Figure 1). Using log10-transformed data with the generalized estimating equation model, we showed that platelet count and leukopenia recovery were delayed in the co-infection group compared with the single-infection group (p = 0.045 and p = 0.027, respectively). The generalized estimating equation model also showed that the co-infection group had higher levels of serum creatine kinase (p = 0.047) and lactate dehydrogenase (p = 0.022) during those recovery processes.
Figure 2

Figure 2. Dynamic profiles for severe fever with thrombocytopenia syndrome virus (SFTSV) RNA and SFTSV-specific IgG in hospitalized patients with SFTSV infection only or with SFTSV and spotted fever group rickettsiae co-infection, China,...
Based on the dynamic patterns at 2-day intervals, virus loads in the single-infection group peaked at day 5 after symptom onset and gradually decreased thereafter. Virus loads in the co-infection group peaked at day 7 and then deceased at a lower rate than that for the single-infection group after we adjusted for sex, age, and time from symptom onset to hospital admission (p = 0.028) (Figure 2, panel A).
At weeks 1 and 2 after symptom onset, SFTSV-specific IgG titers and positivity rates were not significantly different between the 2 groups (Figure 2, panels C, D). At week 3, the co-infection group had a significantly lower rate of SFTSV positivity (p = 0.007). Antibody titers at week 4 were not significantly different between the groups (Figure 2, panel C).
We conducted laboratory testing for 34 patients with SFTSV–SFGR co-infection, 30 sex- and age-matched patients with SFTS only, and 25 controls who were negative for both pathogens by molecular and antibody testing. Levels of interleukin (IL)–1 receptor agonist, IL-8–10, IL-17, interferon-γ, monocyte chemoattractant protein 1, monocyte chemoattractant protein α1, granulocyte colony-stimulating factor, fibroblast growth factors, and tumor necrosis factor–α were similar in the single-infection and co-infection groups and significantly elevated compared with levels in the control group (online Technical Appendix Figure). IL-6 and IL-15 levels were elevated in both infection groups, but they were significantly higher in the SFTSV single-infection group. Platelet-derived growth factor–BB and RANTES (regulated on activation, normal T cell expressed and secreted) were decreased in both groups, but we observed intergroup differences only for RANTES.
Altogether, 87 (10.6%) patients died. The case-fatality rate in the co-infection group (16.9% [13/77]) was insignificantly higher than that in the single-infection group (9.9% [74/746]) (p = 0.058). The association between co-infection and higher case-fatality rate was significant after adjustment for sex, age, and interval from disease onset to hospital admission (odds ratio 1.992, 95% CI 1.025–3.873; p = 0.042) (Technical Appendix Table 4).
Our retrospective investigation in an SFTSV-endemic region of China identified SFTSV–SFGR co-infection in ≈8.5% of SFTSV-infected patients and a higher frequency of fatal outcome and delayed recuperation in the co-infected patients. These findings highlight the importance of considering SFGR infection in the differential diagnosis for patients in SFTSV-endemic regions.
SFTSV infection can cause a wide variety of signs and symptoms, ranging from influenza-like illness to more severe complications and even life-threatening disease (7). Complications usually involve neurologic and hemorrhagic manifestations, which can progress to multiple organ dysfunction in critically ill patients. Rickettsial infections are clinically difficult to distinguish from many virus infections (8), and our results showed that symptoms common to SFTSV- and SFGR-infected patients (e.g., influenza-like illness, gastrointestinal symptoms) are not intensified in co-infected patients. In contrast, less common hemorrhagic signs, especially gastrointestinal hemorrhages, are exacerbated in co-infected patients. Previous studies have shown that in patients with SFTS, blood coagulation parameters are prolonged, as characterized by activated partial thromboplastin time and thrombin time (9,10). Thrombocytopenia, a common laboratory finding in patients with SFTS, can contribute to hemorrhage, and hemorrhagic signs have also been observed in patients infected with SFGR species (e.g., R. rickettsii and R. conorii) (12–14); however, SFGR mainly invade the vascular endothelial cells, causing vascular inflammation and increased vascular permeability (11). Also, based on prolonged thrombocytopenia and longer prothrombin times that have been observed in co-infected persons, we hypothesize that the additive effect from 2 pathogens might lead to aggravated hemorrhage.
Doxycycline is the recommended therapeutic regimen for rickettsia infection (15) and could be administered in cases of SFTSV–SFGR co-infection. From a public health perspective, intensified efforts should be made to detect SFTSV–SFGR co-infection in regions where H. longicornis ticks predominate and carry both SFTSV and SFGR.
Dr. Lu is an epidemiologist in the School of Public Health, Peking University. His research interests are epidemiology of emerging infectious diseases.
Acknowledgments
This study was supported by the Natural Science Foundation of China (81222037, 81473023), the China Mega-Project for Infectious Diseases grants (2013ZX10004-202), and the Youth Talent Support Program by School of Public Health, Peking University. The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
The authors had the following roles in the study and preparation of the manuscript: Q.-B.L., W.L., and W.-C.C. conceived and designed the experiments; Q.-B.L., H.L., P.-H.Z., N.C., Y.-D.F., X.-M.C., J.-G.H., C.-T.G., and X.-A.Z. performed the experiments; Q.-B.L., H.L., P.-H.Z., N.C., and W.L. analyzed the data; N.C. and Z.-D.Y. contributed materials; and Q.-B.L., H.L., P.-H.Z., N.C., and W.L. prepared the manuscript.
References
- Swanson SJ, Neitzel D, Reed KD, Belongia EA. Coinfections acquired from ixodes ticks. Clin Microbiol Rev. 2006;19:708–27.DOIPubMedGoogle Scholar
- Liu K, Zhou H, Sun RX, Yao HW, Li Y, Wang LP, A national assessment of the epidemiology of severe fever with thrombocytopenia syndrome, China. Sci Rep. 2015;5:9679.DOIPubMedGoogle Scholar
- Liu W, Li H, Lu QB, Cui N, Yang ZD, Hu JG, Candidatus Rickettsia tarasevichiae infection in eastern central China: a case series. Ann Intern Med. 2016;164:641–8.DOIPubMedGoogle Scholar
- Zou Y, Wang Q, Fu Z, Liu P, Jin H, Yang H, Detection of spotted fever group Rickettsia in Haemaphysalis longicornis from Hebei Province, China. J Parasitol. 2011;97:960–2.DOIPubMedGoogle Scholar
- Luo LM, Zhao L, Wen HL, Zhang ZT, Liu JW, Fang LZ, Haemaphysalis longicornis ticks as reservoir and vector of severe fever with thrombocytopenia syndrome virus in China. Emerg Infect Dis. 2015;21:1770–6.DOIPubMedGoogle Scholar
- Liu W, Lu QB, Cui N, Li H, Wang LY, Liu K, Case-fatality ratio and effectiveness of ribavirin therapy among hospitalized patients in china who had severe fever with thrombocytopenia syndrome. Clin Infect Dis. 2013;57:1292–9.DOIPubMedGoogle Scholar
- Liu Q, He B, Huang SY, Wei F, Zhu XQ. Severe fever with thrombocytopenia syndrome, an emerging tick-borne zoonosis. Lancet Infect Dis. 2014;14:763–72.DOIPubMedGoogle Scholar
- Walker DH, Paddock CD, Dumler JS. Emerging and re-emerging tick-transmitted rickettsial and ehrlichial infections. Med Clin North Am. 2008;92:1345–61, x.DOIPubMedGoogle Scholar
- Zhang YZ, He YW, Dai YA, Xiong Y, Zheng H, Zhou DJ, Hemorrhagic fever caused by a novel Bunyavirus in China: pathogenesis and correlates of fatal outcome. Clin Infect Dis. 2012;54:527–33.DOIPubMedGoogle Scholar
- Deng B, Zhou B, Zhang S, Zhu Y, Han L, Geng Y, Clinical features and factors associated with severity and fatality among patients with severe fever with thrombocytopenia syndrome Bunyavirus infection in Northeast China. PLoS One. 2013;8:e80802.DOIPubMedGoogle Scholar
- Walker DH, Ismail N. Emerging and re-emerging rickettsioses: endothelial cell infection and early disease events. Nat Rev Microbiol. 2008;6:375–86.DOIPubMedGoogle Scholar
- de Almeida DN, Favacho AR, Rozental T, Barcaui H, Guterres A, Gomes R, Fatal spotted fever group rickettsiosis due to Rickettsia conorii conorii mimicking a hemorrhagic viral fever in a South African traveler in Brazil. Ticks Tick Borne Dis. 2010;1:149–50.DOIPubMedGoogle Scholar
- Maleev VV, Galimzianov KM, Lazareva EN, Poliakova AM, Astrina OS, Kudriavtsev VA, [Hemostatic disorders and their implication in the pathogenesis of Astrakhan rickettsial fever] [in Russian]. Ter Arkh. 2009;81:32–5.PubMedGoogle Scholar
- Centers for Disease Control and Prevention (CDC). Fatal cases of Rocky Mountain spotted fever in family clusters—three states, 2003. MMWR Morb Mortal Wkly Rep. 2004;53:407–10.PubMedGoogle Scholar
- Parola P, Raoult D. Ticks and tickborne bacterial diseases in humans: an emerging infectious threat. Clin Infect Dis. 2001;32:897–928.DOIPubMedGoogle Scholar
Figures
Table
Cite This Article1These authors contributed equally to this article.
Table of Contents – Volume 22, Number 11—November 2016
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Wei Liu, State Key Laboratory of Pathogen and Biosecurity, Beijing Institute of Microbiology and Epidemiology, 20 Dong-Da St, Fengtai District, Beijing 100071, China
Top