Volume 30, Number 5—May 2024
Research Letter
Reemergence of Bordetella parapertussis, United States, 2019–2023
Abstract
To determine changes in Bordetella pertussis and B. parapertussis detection rates, we analyzed 1.43 million respiratory multiplex PCR test results from US facilities from 2019 through mid-2023. From mid-2022 through mid-2023, Bordetella spp. detection increased 8.5-fold; 95% of detections were B. parapertussis. While B. parapertussis rates increased, B. pertussis rates decreased.
Whooping cough is a highly contagious, acute, respiratory illness caused by Bordetella spp. bacteria, primarily B. pertussis and B. parapertussis, and may be associated with complications such as pneumonia (1,2). Unlike B. pertussis, B. parapertussis is not notifiable in the United States because it is thought to be less prevalent and to cause milder symptoms than B. pertussis (1,2). Although isolation of B. parapertussis was uncommon in the United States before 2005, it has since been suggested that B. parapertussis infections are more common than previously recognized and may contribute to cases thought to result from vaccine failure (1,3). Our objective with this study was to detect recent changes in B. pertussis and B. parapertussis detection rates by using a cloud-based near real-time surveillance network.
We analyzed >1.43 million multiplex PCR results from 125 US facilities for January 1, 2019–July 31, 2023, for detection of B. pertussis or B. parapertussis (Table). Information on clinical manifestations, patient demographics, and confirmatory testing were not known. Facilities were primarily reference laboratories or hospitals, 12 of which were pediatric or contained a pediatric site, and all facilities used the BIOFIRE FILMARRAY Respiratory 2 (RP2) Panel, the BIOFIRE Respiratory 2.1 (RP2.1) Panel (bioMérieux, https://www.biomerieux.com), or both (4,5). The RP2 and RP2.1 tests detect nucleic acid of 21 (RP2) or 22 (RP2.1) pathogens commonly associated with respiratory infections and are identical, except the RP2.1 test can also detect SARS-CoV-2. Both tests detect B. pertussis (limit of detection of 1.0 × 103 CFU/mL) and B. parapertussis (limit of detection 4.1 × 101 CFU/mL) (5). Deidentified patient test results were captured by the BIOFIRE Syndromic Trends database, a cloud-based pathogen surveillance network (6). We excluded suspected verification, quality control, and proficiency tests (6).
Figure
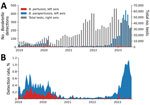
Figure. Bordetalla pertussis and B. parapertussis detection count and detection rates, January 2019–July 2023. A) Total number of tests and number of tests positive for B. pertussis...
We determined the total number of tests in the database and the number of those tests that detected B. pertussis or B. parapertussis, aggregated monthly (Figure, panel A), and detection rates (3-week centered rolling average) for B. pertussis and B. parapertussis (stacked) (Figure, panel B). During January 1, 2019–March 11, 2020 (before the COVID-19 pandemic), we observed that in the United States, the average (95% binomial CI) B. pertussis detection rates (0.14% [95% CI 0.12%–0.16%]) were slightly lower than the B. parapertussis detection rates (0.21% [95% CI 0.18%–0.23%]). From mid-2020 through late 2022, the detection rates of B. pertussis and B. parapertussis declined significantly; the combined rate remained <0.20%. In 2023 (January–July), we observed a marked increase in B. parapertussis detections; average detection rate was 0.65% (95% CI 0.62%–0.68%) and peaked mid-June at 1.3% (95% CI 1.1%–1.6%). We did not observe a similar increase in B. pertussis detections, for which the average detection rate in 2023 was 0.03% (95% CI 0.02%–0.04%).
Comparing recent (January 2023–July 2023) rates to rates from a commensurate prepandemic time frame (January 2019–July 2019), we observed an increase of 0.44% (95% CI 0.39%–0.49%) for B. parapertussis and a decrease of 0.12% (95% CI 0.09%–0.16%) for B. pertussis. Those findings lend evidence to a significant (p<0.001) national B. parapertussis increase and B. pertussis decrease; similar trends were observed in each US Census region. Of the 23 facilities with data for both time frames, the B. parapertussis detection rate increased for 20 facilities.
Co-detection of B. pertussis and B. parapertussis in the same test was rare, observed in only 9 tests (0.03% of tests positive for either B. pertussis or B. parapertussis) (Appendix Table). However, a virus was co-detected with 47.1% (95% CI 42.5%–51.7%) of B. pertussis and 66.2% (95% CI 64.4%–68.0%) of B. parapertussis detections.
In summary, we found that 95% of Bordetella spp. detected in the last year of the study (July 2022– July 2023) were B. parapertussis. The observed high incidence of virus co-detections along with previous data that found that clinical infection developed in <5% of those with B. parapertussis (compared with 75% of those with B. pertussis) may suggest that many of the observed B. parapertussis detections were subclinical (7). Although the reason behind the observed increase in B. parapertussis detections is unknown, Bhattacharyya et al. suggested that the erratic dynamics of whooping cough could be explained by interactions of B. pertussis and B. parapertussis, which oscillate out of phase through age-dependent convalescence (8). It is possible that secondary effects of the COVID-19 pandemic, such as decreased population immunity, affected this interaction, because incidence of many other respiratory illnesses also decreased during the pandemic, followed by atypical prevalence (9).
Testing and near real-time surveillance of B. parapertussis are needed to enhance prompt response to clinical outbreaks and contamination events, both of which have been reported (1,10). Determining the clinical implications of the observed B. parapertussis surge may help inform patient management and public health action.
Dr. Noble is a data scientist at bioMérieux, Salt Lake City, Utah. Her research interests include syndromic testing and spatiotemporal trends of infectious diseases.
Acknowledgments
The data obtained by bioMérieux are subject to the terms and conditions of a data-use agreement by and between bioMérieux and each facility participating in the BIOFIRE Syndromic Trends program. If a dataset is requested, bioMérieux will review such request internally to ensure that any disclosure does not conflict with bioMérieux obligations and restrictions set forth in the data-use agreement. Code available upon reasonable request.
All authors are employees of bioMérieux.
References
- Watanabe M, Nagai M. Whooping cough due to Bordetella parapertussis: an unresolved problem. Expert Rev Anti Infect Ther. 2004;2:447–54. DOIPubMedGoogle Scholar
- Faulkner A, Skoff TH, Martin SW, Cassiday PK, Tondella ML, Liang JL. Chapter 10: Pertussis. In: Manual for the surveillance of vaccine-preventable diseases [cited 2024 Apr 10]. A https://www.cdc.gov/vaccines/pubs/surv-manual/chpt10-pertussis.html
- Cherry JD, Seaton BL. Patterns of Bordetella parapertussis respiratory illnesses: 2008–2010. Clin Infect Dis. 2012;54:534–7. DOIPubMedGoogle Scholar
- Leber AL, Everhart K, Daly JA, Hopper A, Harrington A, Schreckenberger P, et al. Multicenter evaluation of BioFire FilmArray respiratory panel 2 for detection of viruses and bacteria in nasopharyngeal swab samples. J Clin Microbiol. 2018;56:e01945–17. DOIPubMedGoogle Scholar
- BioFire Diagnostics LLC BioFire® Respiratory Panel 2.1 (RP2.1) de novo instructions for use. 2021 [cited 2024 Jan 12]. https://www.biofiredx.qarad.eifu.online/ITI/US/all?keycode=ITI0105
- Meyers L, Ginocchio CC, Faucett AN, Nolte FS, Gesteland PH, Leber A, et al. Automated real-time collection of pathogen-specific diagnostic data: syndromic infectious disease epidemiology. JMIR Public Health Surveill. 2018;4:
e59 . DOIPubMedGoogle Scholar - Lautrop H. Epidemics of parapertussis. 20 years’ observations in Denmark. Lancet. 1971;297:1195–8. DOIPubMedGoogle Scholar
- Bhattacharyya S, Ferrari MJ, Bjørnstad ON. Species interactions may help explain the erratic periodicity of whooping cough dynamics. Epidemics. 2018;23:64–70. DOIPubMedGoogle Scholar
- Shaw D, Abad R, Amin-Chowdhury Z, Bautista A, Bennett D, Broughton K, et al. Trends in invasive bacterial diseases during the first 2 years of the COVID-19 pandemic: analyses of prospective surveillance data from 30 countries and territories in the IRIS Consortium. Lancet Digit Health. 2023;5:e582–93. DOIPubMedGoogle Scholar
- Flipse J, Tromp AT, Bosman J, Ten Hove C, Beks H, Kortbeek T, et al. Pseudo-outbreak of Bordetella parapertussis caused by contaminated swabs in the Netherlands. Emerg Infect Dis. 2022;28:890–2. DOIPubMedGoogle Scholar
Figure
Table
Cite This ArticleOriginal Publication Date: April 12, 2024
Table of Contents – Volume 30, Number 5—May 2024
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Brooklyn A. Noble, bioMérieux, 1201 S 4800 W, Salt Lake City, UT 84104, USA
Top