Volume 11, Number 1—January 2005
Research
Malassezia pachydermatis Carriage in Dog Owners
Cite This Article
Citation for Media
Abstract
Yeasts of the genus Malassezia serve as both commensal microorganisms and pathogens on the skin of humans and domestic animals. Although rare, cases of life-threatening fungemia in people have been attributed to Malassezia pachydermatis, for which dogs are a natural host. Zoonotic transfer has been documented from dogs to immunocompromised patients by healthcare workers who own dogs. We investigated the role of pet dogs as risk factors for mechanical carriage of M. pachydermatis on human hands. Dogs and their owners were sampled as pairs, by fungal culture and nested polymerase chain reaction (PCR). Although fungal culture was not a reliable means by which to detect carriage of the yeast on human hands, PCR identified M. pachydermatis on most (≈93%) human participants. Human carriage of ubiquitous opportunistic pathogens such as M. pachydermatis underscores the importance of good hand hygiene by healthcare professionals.
Yeasts of the genus Malassezia, part of the normal cutaneous microflora of mammals, can cause life-threatening fungemia and other nosocomial infections in immunocompromised humans, especially in preterm neonates (1–3). While disease in humans is most commonly caused by Malassezia furfur, a commensal of human skin (4), it has also resulted from M. pachydermatis, for which dogs are a natural host (5–8). In some cases, the sources of human infections have been traced to pet dogs owned by healthcare workers (9).
In normal dogs with healthy skin, M. pachydermatis colonizes the stratum corneum in very low numbers (10). In dogs with allergic skin disease, however, the numbers of M. pachydermatis may increase dramatically on the skin and within the ear canals (11–13). The potential for human exposure to the organism is therefore quite great. While no evidence has shown that dogs represent an overt health concern to immunocompromised humans, the increasing incidence of immune suppression in humans worldwide suggests that a survey of the zoonotic potential of this organism is relevant to modern hospital hygiene practices.
We hypothesized that mechanical transfer of M. pachydermatis from the inflamed skin of dogs with M. pachydermatis infection to the healthy skin of humans occurs commonly. We also hypothesized that atopic dermatitis of dogs, which is a widely documented risk factor for M. pachydermatis infection, would be a risk factor for human carriage. The purpose of this study was to evaluate the prevalence of M. pachydermatis in dogs and their owners as determined by microbiologic culture and polymerase chain reaction (PCR). The ultimate goal was to assess whether pet owners could be reservoirs for mechanical transfer of the organism.
Study Population
Approvals for privately owned animal use and sampling of human participants were obtained from the University of Pennsylvania’s Institutional Animal Care and Use Committee and the biomedical institutional review board, respectively, and informed consent was obtained from participants.
Dogs referred to the Dermatology and Allergy Service of the Matthew J. Ryan Veterinary Hospital of the University of Pennsylvania (VHUP) for evaluation of allergic skin or ear canal disease were screened for secondary M. pachydermatis overgrowth (i.e., infection, commonly referred to as malassezia dermatitis or malassezia otitis) by using the tape strip and ear swab methods described below. Dogs with positive cytologic results and their human companions were recruited for the disease group.
A control group of healthy dogs and their human companions were recruited from the faculty, staff, and students at the VHUP. Samples were taken from dogs with normal skin and ear canals (defined as no episodes of skin disease in the preceding calendar year and no evidence of inflammation at the time of sampling) and their human companions by using the same techniques as for the disease group.
Cytology
The cytologic collection technique used for skin was the tape strip method (14). A piece of clear cellophane tape (5 cm x 2 cm) was applied to the surface of the skin 2 times in succession, removed, stained with a modified Wright’s stain (Diff Quik, Dade Behring, Deerfield, IL), and applied to a glass slide for microscopic analysis. From dogs with atopic dermatitis, inflamed skin, which was typically alopecic from self-trauma due to pruritus, was sampled. One or more of the following regions were sampled from each dog: axilla, groin, chin, ventral neck fold, paronychium, and interdigital spaces (dorsal or plantar) according to clinical signs. From dogs with ear canal infections, cotton-tipped swabs of ear canal exudates were collected and streaked onto glass slides, which were then heat fixed and stained.
All slides were examined at 1,000x (high power under oil immersion) magnification. This technique allows for microscopic visualization of any microorganisms that reside on the surface of the skin or within the ear canal cerumen. When a minimum number of yeast cells per oil immersion field (oif) was exceeded (>1 yeast/oif on the skin, >5 yeast/oif in ear canal exudates) (10,15,16), excessive colonization by the organism (i.e., infection) was diagnosed, and these dogs were assigned to the disease group.
Microbiologic Analysis
For affected dogs, a tape strip was used to sample a positive skin site (an area adjacent to a site positive for yeast), and sterile cotton-tipped swabs were used to sample ear exudates. In healthy control dogs, only the chin and mucocutaneous junction of the lower lip were sampled, since this area is commonly colonized by M. pachydermatis (10). In the human companions, a single tape strip was used to sample the palms of both hands. To participate, each participant must have abstained from handwashing for at least 1 hour before sampling and must have handled the dog within that period. Veterinary personnel participating in the healthy control group were sampled at least 48 hours after last contact with a veterinary hospital patient.
Tape strips from each pair of participants were placed over drops of sterile olive oil, adjacent to one another, on the surface of a Sabouraud’s dextrose agar plate. The agar was fortified with a drop of olive oil (source of medium- to long-chain fatty acids) to enhance growth of Malassezia spp., which are lipophilic (10). In cases in which canine ear exudate was sampled rather than skin, the swab was rolled across the surface of the agar incorporating a drop of sterile olive oil.
Plates were incubated at 32°C for up to 7 days. Any fungal colonies isolated were harvested from the tape strips with sterile cotton-tipped swabs and identified cytologically to be yeast by morphologic characteristics. Samples without yeast colonies were discarded. Yeast colonies were then stored at –80°C for future identification of species by polymerase chain reaction (PCR).
PCR
Samples for PCR were obtained from all dogs and their human companions. For dogs with malassezia dermatitis or otitis, a sterile cotton-tipped swab moistened with sterile saline was used to rub an affected area. For healthy control dogs, the chin and mucocutaneous junction of the lower lip was sampled. For human hands, a sterile gauze pad moistened with sterile saline was used to vigorously rub the hands (palms, fingers, and interdigital webbing) (17). Samples were stored in sterile saline at –80°C until used for PCR analysis.
DNA was extracted by using a MasterPure Yeast DNA Purification Kit (Epicentre Technologies, Madison, WI) with the following modifications. The cotton tipped swabs were stored in 1 mL sterile saline. The swabs were brought to room temperature and vortexed briefly. A 200-μL aliquot of saline was then removed from the cryotube and transferred to a sterile 1.5-mL centrifuge tube for DNA extraction. Gauze pads were stored in 10 mL of sterile saline. The pads were also brought to room temperature and were then agitated manually. A 1-mL aliquot was aseptically removed from the bag and transferred to a sterile 1.5-mL centrifuge tube. The tubes were centrifuged for 2 min at 13,000 rpm to pellet all cells, and DNA was extracted as described by the manufacturer.
Species characterization of malassezia DNA was performed by using a nested PCR assay developed by Sugita and colleagues (18). Briefly, organisms are identified with species-specific primers derived from the internal transcribed spacer (ITS) region of the ribosomal RNA (rRNA) gene. After amplification of the ITS region, a small aliquot of the reactant is used in a second PCR to identify the Malassezia species. The protocol devised by Sugita and colleagues can identify 7 of the currently recognized Malassezia species, many of which have been isolated from canine skin. The sensitivity of the assay has been determined by Sugita and colleagues as 1 fg of DNA. As we were specifically interested only in M. pachydermatis for the purposes of this study, DNA samples were amplified with M. pachydermatis-specific primers. DNA from M. pachydermatis ATCC strain 14522 was prepared by American Type Culture Collection and used as a positive control in all reactions.
Statistical Analysis
To determine differences between culture and PCR in detecting M. pachydermatis on humans and dogs, the McNemar test was used. Where applicable, odds ratios (OR) and 95% confidence intervals (CI) were calculated. To determine if the owners of dogs with malassezia dermatitis or otitis were more likely to harbor the yeast than owners of normal dogs, the Fisher exact test was used. Additionally, to assess concordance of culture and PCR results between owner and dog pairs, for both affected and normal groups, the McNemar test was performed. All analyses were performed by using statistical software (StatXact, Version 6, Cytel Software Corp., Cambridge, MA). A p < 0.05 was considered statistically significant.
Figure 1

Figure 1. Rates of detection of Malassezia pachydermatis on canine and human skin by 2 laboratory techniques. A normal group of dogs and a group known to harbor M. pachydermatis infection, paired with...
Fifty healthy dogs and 75 atopic dogs with malassezia dermatitis or otitis and their respective human companions made up the control and affected groups, respectively. Of the control group, 5 (10%) of 50 canine samples were positive for M. pachydermatis growth on lipid-enriched Sabouraud’s dextrose agar, and 3 (6%) of 50 human samples were positive (Figure 1). No differences in rates of isolation were seen (p = 0.6).
Figure 2
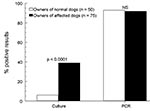
Figure 2. Comparison of rates of detection of Malassezia pachydermatis on the hands of dog owners by 2 laboratory techniques. NS, nonsignificant; PCR, polymerase chain reaction.
Of the affected group, 61 (81.3%) of 75 canine samples were positive for M. pachydermatis, while 4 samples were overgrown with saprophytic molds before yeast colonies had grown, and 10 were negative. Of the human samples from this group, 29 (38.7%) of 75 were positive, while 5 were overgrown with saprophytic molds, and 41 were negative (Figure 1). For the 70 canine-human pairs with complete culture results, the dogs were more likely to have a positive result than their owners (p < 0.0001). Of the 61 dogs with positive cultures, only 49% had a concordantly positive owner (data for individual pairs not shown). However, all positive owners had dogs that were also positive. When comparing detection of M. pachydermatis between owners of normal dogs and owners of affected dogs by culture, the latter were 11.1 times more likely to be positive (95% CI 3.0–59.9, p < 0.0001, Figure 2).
PCR
Of the control group, 43 (86%) of 50 canine samples and 46 (92%) of 50 human samples were positive for M. pachydermatis (Figure 1). All participants (canine or human) with positive culture results were also positive by PCR; however, 38 dogs and 45 humans with negative cultures were positive by PCR. No difference was seen in the rate of detection (p = 0.3) between owner and dog.
Of the affected group, 73 (97.3%) of 75 canine samples and 70 (93.3%) of 75 human samples were positive by PCR for M. pachydermatis (Figure 1). Sixty-eight pairs had concordant positive results, and no negative pairs were found. No differences in rates of detection between the dogs and their owners were seen (p = 0.45). When comparing detection of M. pachydermatis between owners of affected dogs and owners of normal dogs by PCR, no differences (p = 1.0, 93% vs. 92%, respectively) were seen between groups (Figure 2).
Microbiology versus PCR
When comparing PCR to culture, regardless of participant species or disease group, PCR was more likely to detect M. pachydermatis than culture. For dogs, PCR was 24 times more likely to be positive compared to culture (OR = 24, 95% CI 5.9–98.7), whereas for humans, PCR was 80 times more likely to be positive (OR = 80, 95% CI 11.1–574.9).
Yeast organisms of the genus Malassezia are lipophilic fungi that occur as commensal inhabitants of the skin of mammals and birds in very low numbers (19). Ten distinct species are now recognized (20–22), and M. pachydermatis, M. furfur, M. globosa, and M. sympodialis are the best characterized with regard to clinical disease correlations (11–13,23,24). M. pachydermatis is part of the normal cutaneous microflora of dogs and many other mammals (19), while M. furfur, M. globosa, M. sympodialis, and M. restricta reside naturally on the skin of human beings (18,23,25). Lipophilic organisms exhibit the unique capability of using lipid as a source of carbon. All species except M. pachydermatis are entirely lipid dependent. While M. pachydermatis does not exhibit an absolute requirement for lipid, its growth is still enhanced by the addition of lipid substrates to culture media (20).
In normal dogs with healthy skin, M. pachydermatis can routinely be isolated by fungal culture, but proving the presence of the organism by skin surface cytology can be difficult (10). In dogs with allergic or seborrheic skin diseases, the homeostasis of the local cutaneous microenvironment is disrupted by inflammation and increased levels of moisture or sebum (26,27). Under these conditions, the number of M. pachydermatis organisms on the skin and in the ear canals may increase dramatically, making it possible to readily identify the organism with rapid cytologic screening (11–13). Atopic dermatitis may affect up to 10% of the canine population and is the most common reason that dogs are brought to our dermatology clinic for examination. It is also the most common predisposing factor for M. pachydermatis infections of the skin and ear canals. The potential for exposure of human beings to the organism is therefore great.
In human beings, especially preterm neonates and immunocompromised adults, M. furfur has been shown to cause a systemic bloodborne infection of patients receiving lipid-rich, parenteral nutritional infusions by catheter (4). Of zoonotic concern, M. pachydermatis has been documented to cause fungemia in similar patient populations (7,9); however, since this species is not lipid-restricted in its growth, lipid infusion is not a prerequisite for infection (9). Chang and colleagues suggested that the source of an outbreak in an intensive care nursery was pet dogs owned by nursing staff who worked in the neonatal intensive care unit (NICU). A single strain of M. pachydermatis, as determined by pulsed-field gel electrophoresis, was isolated from infants, the hands of a nurse, and from 3 dogs owned by other healthcare workers in the NICU. This observation suggested that M. pachydermatis could represent an emerging zoonotic pathogen.
A limited number of studies have investigated the prevalence of M. pachydermatis carriage by human beings. One report identified carriage of very low numbers of the organism on the scalp and palms of 24 (12%) of 200 normal volunteers from whom samples were collected by a washing technique for fungal culture, with subsequent speciation of yeast by biochemical methods (28). Although an association with pet ownership was speculated, such information was not collected from the participants. More recent reports have provided much lower estimates of human carriage. One report suggested that M. pachydermatis is present on the skin of <1% of normal persons but may be found in ≈2% of dermatitis patients (patients sampled by a swab technique for fungal culture) (23), while a second study failed to isolate the organism from either healthy human volunteers or dermatitis patients when application of transparent dressings for subsequent PCR detection was used as the sampling technique (22). To date, no single study has directly and systematically addressed the relationship between M. pachydermatis carriage on human skin and dog ownership. In the epidemiologic investigation of the NICU outbreak mentioned previously, a total of 53 pets (dogs, cats, and horses) were surveyed, and 12 (31%) of the 39 dogs were positive for M. pachydermatis, 3 of which matched the outbreak strain. However, only 1 of 9 nurses, who was not a pet owner, was positive for M. pachydermatis (9).
The cytologic and microbiologic results from dogs in this study mirror the literature regarding M. pachydermatis carriage on the skin of normal and atopic dogs (10,15,29). Ten dogs identified with malassezia infection by cytology were negative on culture. While this finding seems counterintuitive, it is not unusual in our clinical experience. The organism may have failed to grow because of suboptimal culture conditions or nonviable yeast cells. All positive cultures were confirmed to be M. pachydermatis by PCR, which confirms our ability to identify the species properly by cytology.
We were significantly less likely to isolate the organism from the skin of normal dogs than from atopic dogs in our study, but this bias was deliberate, since samples for culture were taken from sites that were known to be positive from rapid cytologic screening. However, when PCR was used, no significant difference was seen in detection rates, which reflects the commensal status of the organism on canine skin.
If the culture technique alone had been used, the significantly higher rate of yeast isolation from the hands of the companions of the disease group versus the control group (38.7% vs. 6%) would have supported our hypothesis that active malassezia infection of canine skin or ear canals is a risk factor for human carriage. However, when PCR was used as the detection technique, no significant difference was seen between detection rates on the hands of the 2 human groups (93.3% vs. 94%), which caused us to reject this hypothesis.
As part of the normal microflora of canine skin, M. pachydermatis is expected to be detectable by a technique as sensitive as PCR, even from sample sites that do not yield colony growth on culture. With our handwashing and canine skin and ear canal swabbing techniques, a larger surface area was sampled, especially on human hands, and the PCR was presumably able to detect low cell numbers within a large sample aliquot. The culture technique we used for human hands appears to be inadequate for screening purposes; however, we do not know the number or density of viable yeast cells on human hands that may be required to nosocomially spread infection in a clinical setting.
Since reports of M. pachydermatis-associated septicemia in humans are relatively scarce, our conclusion is that mechanical carriage of the organism is of low risk to public health. Dogs are commonly used for their therapeutic benefits in clinical settings, such as cancer therapy support groups for children and the elderly, and in psychiatric care facilities. The benefits of canine interaction have been documented (30). Advice to pet owners is available at http://www.cdc.gov/healthypets.
In intensive care units, where nosocomial infections are especially problematic, good handwashing practices among healthcare workers are imperative. Unfortunately, little is known about handwashing agents and techniques (e.g., contact time) that will effectively eliminate carriage of malassezia yeast from human hands, and disparate evidence is presented in the literature. In 1 report, improved handwashing practices seemed to eliminate an endemic problem with M. pachydermatis infections in a NICU (9), while in another, elimination of M. furfur from the surfaces of equipment was not achieved with routine hygienic measures (7).
Dr. Morris is an assistant professor and chief of dermatology and allergy at the University of Pennsylvania’s School of Veterinary Medicine. His primary research interests include infectious and zoonotic skin diseases and have focused on the host (canine) immune response to the yeast Malassezia pachydermatis.
Acknowledgment
This work was funded in its entirety by a grant from the American Academy of Veterinary Dermatology.
References
- Marcon MJ, Powell DA. Human infections due to Malassezia spp. Clin Microbiol Rev. 1992;5:101–19.PubMedGoogle Scholar
- Morrison VA, Weisdorf DJ. The spectrum of Malassezia infections in the bone marrow transplant population. Bone Marrow Transplant. 2000;26:645–8. DOIPubMedGoogle Scholar
- Archer-Dubon C, Icaza-Chivez ME, Orozco-Topete R, Reyes E, Baez-Martinez R, Ponce de Leon S. An epidemic outbreak of Malassezia folliculitis in three adult patients in an intensive care unit: a previously unrecognized nosocomial infection. Int J Dermatol. 1999;38:453–6. DOIPubMedGoogle Scholar
- Dankner WM, Spector SA, Furer J, Davis CE. Malassezia fungemia in neonates and adults: complication of hyperalimentation. Rev Infect Dis. 1987;9:743–53. DOIPubMedGoogle Scholar
- Chryssanthou E, Broberger U, Petrini B. Malassezia pachydermatis fungemia in a neonatal intensive care unit. Acta Paediatr. 2001;90:323–7. DOIPubMedGoogle Scholar
- Mickelsen PA, Viano-Paulson MC, Stevens DA, Diaz PS. Clinical and microbiological features of infection with Malassezia pachydermatis in high-risk infants. J Infect Dis. 1988;157:1163–8. DOIPubMedGoogle Scholar
- vanBelkum A, Boekhout T, Bosboom R. Monitoring spread of Malassezia infections in neonatal intensive care unit by PCR-mediated genetic typing. J Clin Microbiol. 1994;32:2528–32.PubMedGoogle Scholar
- Welbel SF, McNeil MM, Pramanik A, Silberman R, Oberle AD, Midgley G, Nosocomial Malassezia pachydermatis bloodstream infections in a neonatal intensive care unit. Pediatr Infect Dis J. 1994;13:104–8. DOIPubMedGoogle Scholar
- Chang HJ, Miller HL, Watkins N, Arduino MJ, Ashford DA, Midgley G, An epidemic of Malassezia pachydermatis in an intensive care nursery associated with colonization of health care workers’ pet dogs. N Engl J Med. 1998;338:706–11. DOIPubMedGoogle Scholar
- Kennis RA, Rosser EJ Jr, Olivier NB. Quantity and distribution of Malassezia organisms on the skin of clinically normal dogs. J Am Vet Med Assoc. 1996;208:1048–51.PubMedGoogle Scholar
- Matousek JL, Campbell KL. Malassezia dermatitis. Compend Contin Educ Small Anim Pract. 2002;24:224–31.
- Morris DO. Malassezia dermatitis and otitis. In: Campbell KA, editor. Veterinary clinics of North America: small animal practice. Philadelphia: W.B. Saunders Co.; 1999. p. 1303–10.
- Muse R. Malassezia dermatitis. In: Bonagura JD, editor. Kirk’s current veterinary therapy XIII. Philadelphia: W.B. Saunders Co.; 2000. p. 574–7.
- Omodo-Eluk AJ, Baker KP, Fuller H. Comparison of two sampling techniques for the detection of Malassezia pachydermatis on the skin of dogs with chronic dermatitis. Vet J. 2003;165:119–24. DOIPubMedGoogle Scholar
- Morris DO, Olivier NB, Rosser EJ. Type-1 hypersensitivity reactions to Malassezia pachydermatis extracts in atopic dogs. Am J Vet Res. 1998;59:836–41.PubMedGoogle Scholar
- Cole LK, Kwochka KW, Kowalski JJ, Hillier A. Microbial flora and antimicrobial susceptibility patterns of isolated pathogens from the horizontal ear canal and middle ear in dogs with otitis media. J Am Vet Med Assoc. 1998;212:534–8.PubMedGoogle Scholar
- Petersen NJ, Collins DE, Marshall JH. A microbiological assay technique for hands. Health Lab Sci. 1973;10:18–22.PubMedGoogle Scholar
- Sugita T, Suto H, Unno T, Tsubol R, Ogawa H, Shinoda T, Molecular analysis of Malassezia microflora on the skin of atopic dermatitis patients and healthy subjects. J Clin Microbiol. 2001;39:3486–90. DOIPubMedGoogle Scholar
- Akerstedt J, Vollset I. Malassezia pachydermatis with special reference to canine skin disease. Br Vet J. 1996;152:269–81. DOIPubMedGoogle Scholar
- Gueho E, Midgley G, Guillot J. The genus Malassezia with description of four new species. Antonie van Leeuwenhoek. 1996;69:337–55. DOIPubMedGoogle Scholar
- Nell A, James SA, Bond CJ, Hunt B, Herrtage ME. Identification and distribution of a novel Malassezia species yeast on normal equine skin. Vet Rec. 2002;150:395–8. DOIPubMedGoogle Scholar
- Sugita T, Takashima M, Kodama M, Tsuboi R, Nishikawa A. Description of a new species, Malassezia japonica, and its detection in patients with atopic dermatitis and healthy subjects. J Clin Microbiol. 2003;41:4695–9. DOIPubMedGoogle Scholar
- Nakabayashi A, Sei Y, Guillot J. Identification of Malassezia species isolated from patients with seborrhoeic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Med Mycol. 2000;38:337–41.PubMedGoogle Scholar
- Johansson C, Sandstrom MH, Bartosik J, Sarnhult T, Christiansen J, Zargari A, Atopy patch test reactions to Malassezia allergens differentiate subgroups of atopic dermatitis patients. Br J Dermatol. 2003;148:479–88. DOIPubMedGoogle Scholar
- Bernier V, Weill FX, Hirigoyen V, Elleau C, Feyler A, Labreze C, Skin colonization by Malassezia species in neonates: a prospective study and relationship with neonatal cephalic pustulosis. Arch Dermatol. 2002;138:215–8. DOIPubMedGoogle Scholar
- Plant JD, Rosencrantz W, Griffin CE. Factors associated with and prevalence of high Malassezia pachydermatis numbers on dog skin. J Am Vet Med Assoc. 1992;201:879–82.PubMedGoogle Scholar
- Bond R, Ferguson EA, Curtis CF, Craig JM, Lloyd DH. Factors associated with elevated cutaneous Malassezia pachydermatis populations in dogs with pruritic skin disease. J Small Anim Pract. 1996;37:103–7. DOIPubMedGoogle Scholar
- Bandhaya M. The distribution of Malassezia furfur and Malassezia pachydermatis on normal human skin. Southeast Asian J Trop Med Public Health. 1993;24:343–6.PubMedGoogle Scholar
- Morris DO, DeBoer DJ. Evaluation of serum obtained from atopic dogs with dermatitis attributable to Malassezia pachydermatis for passive transfer of immediate hypersensitivity to that organism. Am J Vet Res. 2003;64:262–6. DOIPubMedGoogle Scholar
- Fine A, ed. Handbook on animal-assisted therapy: theoretical foundations and guidelines for practice. San Diego: Academic Press; 2000.
Figures
Cite This ArticleTable of Contents – Volume 11, Number 1—January 2005
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Daniel O. Morris, Department of Clinical Studies, School of Veterinary Medicine, University of Pennsylvania, 3900 Delancey St, Philadelphia, PA 19104, USA; fax: 215-573-1789
Top