Volume 18, Number 11—November 2012
Research
Unchanged Severity of Influenza A(H1N1)pdm09 Infection in Children during First Postpandemic Season
Cite This Article
Citation for Media
Abstract
We conducted a nationwide hospital-based prospective study in Germany of influenza A(H1N1)pdm09 cases among children <15 years of age admitted to pediatric intensive care units and related deaths during the 2009–10 pandemic and the 2010–11 postpandemic influenza seasons. We identified 156 eligible patients: 112 in 2009–10 and 44 in 2010–11. Although a shift to younger patients occurred in 2010–11 (median age 3.2 vs. 5.3 years), infants <1 year of age remained the most affected. Underlying immunosuppression was a risk factor for hospital-acquired infections (p = 0.013), which accounted for 14% of cases. Myocarditis was predictive of death (p = 0.006). Of the 156 case-patients, 17% died; the difference between seasons was not significant (p = 0.473). Our findings stress the challenge of preventing severe postpandemic influenza infection in children and the need to prevent nosocomial transmission of influenza virus, especially in immunosuppressed children.
In Germany during the influenza A(H1N1)pdm09 pandemic, there were ≈1,070,000 influenza-related medical consultations and ≈1,800 hospitalizations for children 0–14 years of age during October 12, 2009–January 15, 2010, as determined using data provided by the German syndromic surveillance system for acute respiratory infections (1). Moreover, 29 laboratory-confirmed A(H1N1)pdm09 infection–related deaths in children were notified through the mandatory German surveillance system for infectious diseases (2). The highest number of notified hospitalizations and deaths were among children 10–14 years of age (3,4). In a nationwide hospital-based observational study investigating severely ill children who had been admitted to pediatric intensive care units (PICUs) or had died with laboratory-confirmed A(H1N1)pdm09, we reported a high proportion (75%) of case-patients with underlying risk factors, of which neurodevelopmental disorders were most prevalent (5). In addition, we found that in 10% of the cases, children had acquired their infection while hospitalized and that few had been vaccinated, revealing a need for improving preventive measures to reduce severe disease and adverse outcomes (5).
On August 10, 2010, the general director of the World Health Organization declared the world was no longer in phase 6 of influenza pandemic alert; we were moving into the postpandemic phase (6). Experience from past pandemics suggested that the pandemic virus would gradually take on the behavior of a seasonal influenza virus and circulate for several years. However, in view of the potential for transformation of the virus into a more virulent form (7), as suggested by higher rates of mortality during second pandemic waves in Copenhagen (1918), the United States (1957), and Eurasia (1968–1970) (8,9), the World Health Organization acknowledged the unpredictability of pandemic viruses; recommended continued vigilance; and issued advice on surveillance, vaccination, and prompt clinical management of cases during the postpandemic phase (6).
Little is known about the severity of A(H1N1)pdm09 in children during the first postpandemic season (10). To obtain information on critically ill A(H1N1)pdm09-infected children and to compare risk factors and disease course, outcome, and severity for patients during the pandemic and first postpandemic season, we prospectively and continuously performed a nationwide study in Germany during August 3, 2009–July 29, 2011.
Study Design
We conducted a nationwide prospective observational study in Germany by using the German Survey Center for Rare Pediatric Diseases (ESPED; an established children’s hospitals network comprising all 375 pediatric hospitals in Germany) to identify children <15 years of age admitted to PICUs with confirmed A(H1N1)pdm09 infection and related deaths. Cases and related deaths during August 3, 2009–July 29, 2011 were reported by using a standardized form. In pandemic season 2009–10 (August 3, 2009–August 9, 2010), the case definition included only A(H1N1)pdm09 infection; in postpandemic season 2010–11 (August 10, 2010–July 29, 2011), the case definition included all influenza virus infections.
Data Collection
Figure 1
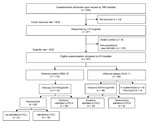
Figure 1. . . . . Overview of study participation and participant groups among severe pediatric cases with A(H1N1)pdm09, Germany, 2009–2011. PCIU, pediatric intensive care unit.
On notification by treating physicians of patients with A(H1N1)pdm09 infection, the ESPED study center distributed and subsequently collected a structured questionnaire, which had been adapted by the authors from an earlier study on seasonal influenza (11). Of 284 distributed questionnaires requested by 186 hospitals, 95% (271/284) were returned to the study center (Figure 1). After excluding 3 questionnaires that had been notified twice and 101 questionnaires for patients who did not meet the case definition, 62% (167/271) of the questionnaires from 83 hospitals remained. Reasons for not meeting the case definition included patient age >15 years and patient not admitted to PICU. In accordance with the case definition, only cases of A(H1N1)pdm09 infection were reported during the pandemic season (2009–10), and 9 cases of influenza A (not further subtyped) and 2 cases of influenza B infection were reported in the postpandemic season (2010–11). Therefore, further analyses were restricted to A(H1N1)pdm09 cases.
The structured questionnaire covered anonymous patient information and information regarding the hospital stay, clinical signs and symptoms, clinical and laboratory findings, specific treatments, status of influenza vaccination, disease complications, and underlying chronic medical conditions (chronic respiratory diseases; cardiac diseases; immunodeficiency; and neurodevelopmental disorders, including developmental delay, cerebral palsy, epilepsy, and other cognitive disorders). Answer categories were predetermined, but free space was designated for respondents to provide information about other diagnoses and coexisting illnesses/medical conditions. Hospital-acquired infection was defined by a date of symptom onset being >2 days after the date of hospital admission; 2 days corresponds with the median incubation time for A(H1N1)pdm09 according to Cao et al. (12). Data were double entered by using EpiData 3.1 software (www.epidata.dk/) in an electronic database.
Data Analysis
Reported values are those for children with available information. Descriptive statistics comprised the calculation of median and interquartile ranges (IQRs) for continuous variables and absolute numbers and proportions (together with 95% binomial exact CIs, when appropriate) for categorical variables. Comparative analyses were based on the Wilcoxon rank-sum test for continuous variables and Fisher exact test for categorical variables. Odds ratios (ORs) and 95% CIs were calculated. Multivariable analysis was performed by using a logistic regression with a stepwise approach to compare cases of hospital-acquired infection with cases of community-acquired infection and survivors with nonsurvivors in PICUs. In doing so, risk factors with a p value <0.2 were considered for multivariable analysis, with the exception of age, sex, and season, which were included in all models. Reported p values are 2-sided, and p<0.05 was considered significant. Statistical analyses were performed by using Stata 11.0 (StataCorp LP, College Station, TX, USA).
Data Protection and Ethics Clearance
Adherence to national data protection laws was approved by the Federal Commissioner for Data Protection and Freedom of Information of Germany. Ethical approval was granted by the Ethics Committee, Charité-Universitätsmedizin, Berlin, Germany.
Comparison of 2009–10 and 2010–11 Seasons
Figure 2

Figure 2. . . Distribution of 136 critically ill children with confirmed A(H1N1)pdm09, by date of disease onset, September 21, 2009–February 22, 2011, Germany. Only cases with available date of symptom onset are...
We identified 156 critically ill children with confirmed A(H1N1)pdm09 infection: 112 in 2009–10 and 44 in 2010–11 (Figure 1). Dates of symptom onset ranged from September 21, 2009, to March 20, 2010, for 2009–10 and from December 20, 2010, to February 22, 2011, for 2010–11 (Figure 2). Cases were reported from 15 of the 16 federal states in Germany during 2009–10 and from 10 during 2010–11.
Figure 3

Figure 3. . . Proportion of critically ill children with A(H1N1)pdm09 by age group and season, Germany.
Figure 4

Figure 4. . . . . Age distribution of the 156 critically ill children with confirmed A(H1N1)pdm09, by season, Germany.
The proportion of boys among case-patients was higher in 2009–10 than 2010–11 (59% vs. 37%, p = 0.02) (Table 1). The median age of case-patients was 5.3 and 3.2 years in 2009–10 and 2010–11, respectively, and differed statistically (p = 0.007) between the 2 seasons. The age distribution in 2010–11 compared with that in 2009–10 was characterized by a markedly higher proportion of children < 2 years of age and a lower proportion of children 10–14 years of age (Figure 3). In both seasons, infants <1 year of age represented the age group with the highest number of cases (Figure 4).
Of the 146 children with available information, 114 (78%) had >1 chronic underlying medical condition; the difference between seasons for these conditions was not statistically significant (Table 1). In both seasons, neurodevelopmental disorders were the most prevalent underlying medical condition. Of the 156 critically ill case-patients, 130 were >6 months age and thus eligible for vaccination against A(H1N1)pdm09 virus; however, for children with available information on vaccination status, only 5 (7%) of 67 vaccine-eligible case-patients had been vaccinated in the 2009–10 season, and none had been vaccinated in the 2010–11 season. Of the 69 total children in both seasons with underlying chronic medical conditions, 64 (93%) had not been vaccinated against A(H1N1)pdm09 virus.
More cases of sepsis were reported during the postpandemic season than during the pandemic season (21% vs. 8%; p = 0.048) (Table 1). Treatment with oseltamivir was used equally (in ≈62% of children) during both seasons. The time to oseltamivir administration after symptom onset (median 4 days) was similar throughout both seasons. The use of catecholamine and mechanical ventilation was more frequent in 2010–11 than in 2009–10, but the difference was not statistically different.
Hospital-acquired Infections
Hospital-acquired infections accounted for 11% (11 of 101) of the cases in 2009–10 and for 23% (8/35) in 2010–11 (p = 0.0931) (Table 1). Of the total study cohort, 14% (19/136) of the patients (9 in a general ward and 10 in a PICU) most likely had hospital-acquired infection. For these case-patients, the median time from hospital admission to symptom onset was 29 days (IQR 12–73 days). The median age for patients with hospital-acquired infection was 1.1 years, and 56% (10/18) were boys (difference not statistically significant between seasons).
The overall case-fatality ratios were 26% (5/19) among patients with hospital-acquired infection and 20% (23/117) among those with community-acquired infection (p = 0.543). Compared with patients with community-acquired infection, those with hospital-acquired infection had more complications, including acute respiratory distress syndrome (ARDS) (OR 2.7, p = 0.054) and sepsis (OR 3.1, p = 0.064), but the differences were not statistically significant (Table 2). In the multivariable model, immunodeficiency (OR 5.9, 95% CI 1.5–23.9; p = 0.013) and mechanical ventilation (OR 8.9, 95% CI 1.1–74.7; p = 0.043) were significantly associated with hospital-acquired infection after adjusting for age, sex, and season.
Case Fatalities Ratios
The case fatality ratio in PICUs did not differ between seasons: 15% (16/106) and 21% (9/44) of PICU case-patients died in 2009–10 and 2010–11, respectively (p = 0.473) (Table 1). For the 2 seasons, 25 of 150 PICU case-patients died, corresponding to a case-fatality ratio of 17% (95% CI 11%–24%). On hospital discharge, 26% (27/104) of the survivors were reported to have possible sequelae or worsening of a pre-existing medical condition.
No statistical differences were found between survivors and nonsurvivors in underlying chronic medical conditions and vaccination status. ARDS (OR 3.2, 95% CI 1.1–9.2, p = 0.029), myocarditis (OR 30.9, 95% CI 2.6–360.7,; p = 0.006), and mechanical ventilation (OR 18.3; 95% CI 1.3–251.6, p = 0.030) were independently associated with a fatal outcome in the multivariable model after adjusting for age, sex, and season (Table 3).
Compared with survivors, nonsurvivors more frequently required mechanical ventilation (p = 0.001) and treatment with catecholamine (p = 0.002); no differences were found in oseltamivir administration (65% vs. 62%, p = 0.8185). Time from symptom onset to oseltamivir uptake did not differ between survivors (median 4 days, IQR 1–6 days) and nonsurvivors (median 4 days, IQR 2–8 days).
During the first postpandemic season, fewer cases of A(H1N1) pdm09 infection were reported, but the severity and outcome of cases did not differ between the pandemic and postpandemic seasons. We further analyzed data from the 2 seasons as 2 outbreak waves of 1 virus and identified a high number of hospital-acquired infections and ARDS and myocarditis as 2 predictors for a fatal outcome.
Compared with the 2009–10 pandemic season, the 2010–11 postpandemic season started later in the winter and had less than half the number of cases. High disease awareness during the pandemic season may have enhanced testing and reporting during 2009–10; thus the reduced case number for 2010–11 should be interpreted with caution. However in the United States, where reporting of influenza-related deaths in children is mandatory, a similar decline in the number of fatal A(H1N1)pdm09-associated cases was noted between the 2009–10 and 2010–11 influenza seasons (282 and 71 deaths among children, respectively) (13). Before the 2009–10 pandemic and similar to the postpandemic season, an average of 82 (range 46–153) children in the United States died each year from seasonal influenza–related illnesses (14). However, in the postpandemic 2010–11 season, different proportions of all circulating influenza subtypes might have led to different numbers of persons exposed to A(H1N1)pdm09, which makes comparisons between seasons and across countries difficult.
For the 2010–11 season, we assumed a more limited number of susceptible persons because exposure to influenza virus during the pandemic might have provided immunologic protection (15–17). This hypothesis is supported by our results showing a shift toward infection in younger age groups in 2010–11. A similar finding was reported in a prospective study of children with A(H1N1)pdm09 infection in a Spanish hospital (median age 7.0 and 0.8 years in 2009–10 and 2010–11, respectively) (10). During both seasons, children <1 year of age were more affected than those in other age groups, and the numbers infected in the 2 seasons were similar; therefore, influenza infection in this immunologically naive age group might always reflect a pandemic-like situation. It remains unexplained why more boys in 2009–10 (59%, 65/111) than in 2010–11 (37%, 16/43) had serious A(H1N1)pdm09 infection, although it has been suggested that the difference in age distribution between the 2 seasons could have influenced the sex distribution (18).
Our results show that case-fatality ratios for the 2 seasons were similar. In Greece (19) and New-Zealand (20), according to the respective national surveillance systems in intensive care unit settings, case-fatality ratios among all age groups were also similar for the 2 seasons. This result is reassuring, in view of concerns of a possible transformation of the strain into a more severe form (7), and is in agreement with the antigenic and genetic homogeneity of the virus since its emergence (21).
In both seasons, we identified a large number of probable hospital-acquired A(H1N1)pdm09 infections. Immunodeficiency, most often reported as acute lymphoblastic leukemia, was associated with hospital-acquired infection, and this underlying chronic medical condition, has also been identified as a risk factor for community-acquired A(H1N1)pdm09 (22,23). Findings from a retrospective hospital-based study investigating the prevalence of respiratory virus infections among children with cancer or HIV infection reported that 40% of the respiratory infections were acquired during the hospital stay, and influenza A virus was the second most prevalent respiratory infection (24). In our study, patients with hospital-acquired infection had more complications, including ARDS and sepsis, than patients with community-acquired infections. However, a significant association between hospital-acquired infection and death was not found, possibly because of the small number of cases, as found by Spaeder et al. (25) in a retrospective cohort study in PICU setting. In this study, hospital acquisition of viral respiratory infection was shown to be associated with an increased risk for death, even after adjusting for chronic medical conditions that predispose to an increased risk for complications from viral illness. Our findings emphasize the need for isolation of and preventive measures for children with immunodeficiency, as reported (26). Preventive measures should include the vaccination of health care workers. Indeed, a survey in Germany showed that only 35% (n = 3,900) of the health care workers in a university hospital setting were vaccinated during the 2010–11 influenza season (27). Studies in earlier seasons showed even lower influenza vaccination rates among health care workers (28).
We identified 25 A(H1N1)pdm09-associated deaths among children admitted to PICUs during the pandemic and postpandemic seasons. ARDS was the most prevalent complication among case-patients who died (60% of cases) and was highly associated with death. Myocarditis was also highly associated with death in children; this finding supports those among adults (29,30) and other findings among A(H1N1)pdm09-infected children (31).
During both seasons, 62% of the children received oseltamivir treatment. This proportion is lower than described in other studies in PICU settings, e.g., 81% in an inception-cohort study in Australia and New Zealand (32), 88% in a US cohort (31), 96% in a retrospective observational multicenter study in Turkey (33), and 100% of children in a retrospective Dutch cohort (34). Observational and random clinical trials have shown the potential of oseltamivir to reduce the length of hospitalization when started <24 hours of illness onset (35,36). The Infectious Diseases Society of America recommends that any person with confirmed or suspected influenza who requires hospitalization receive influenza antiviral therapy, even if the patient enters care >48 hours after illness onset (37). The German Society for Pediatric Infectious Diseases recommends that immunocompetent children without underlying chronic medical conditions should not receive influenza antiviral therapy >48 hours after onset of influenza symptoms (38). Most A(H1N1)pdm09 virus isolates tested worldwide remain sensitive to oseltamivir; thus, strategies to optimize the use of oseltamivir should be considered, and additional evidence should be collected with respect to reduction of nosocomial spread of A(H1N1)pdm09 virus and to potential benefits from late treatment in severely ill children.
We showed that 93% of the children with underlying chronic medical conditions who were eligible for vaccination had not been vaccinated. This finding highlights a need to improve vaccine coverage among this population, for which influenza vaccination is recommended in Germany (39). Children who did not survive received more intensive treatment (mechanical ventilation and catecholamine) than those who survived, and nearly all influenza A viruses tested continue to be antigenically similar to those found in the current trivalent vaccine (40); thus, enhanced prevention in children through vaccination, especially among those with underlying chronic medical conditions, remains a high priority.
Our study is subject to several limitations. Factors such as physicians’ awareness, diagnostic testing, and reporting behavior, which may have had different influences in the 2 seasons, were not assessed. Only children hospitalized in pediatric hospitals were included in the study; however, it can be assumed that critically ill children hospitalized in general hospitals were transferred to pediatric hospitals covered by the ESPED network. In addition, our knowledge of the clinical features of patients was based only on information provided in the structured questionnaires. Ascertainment of underlying chronic medical conditions was not standardized and, thus, may have differed among treating physicians.
During the first postpandemic A(H1N1)pdm09 season, the situation for children with severe A(H1N1)pdm09 disease did not differ from that for children with severe disease during the pandemic. Signs of pulmonary failure or suspected myocarditis in such children should alert health care providers to immediately initiate maximum care, and prevention of nosocomial transmission of influenza virus should be reinforced, especially in immunosuppressed children. The unchanged severity of influenza A(H1N1)pdm09 virus infections in the first postpandemic season (2010–11) and the constant high proportion of possibly hospital-acquired infections stress the challenge of preventing severe cases in children beyond the pandemic situation.
Dr Altmann is epidemiologist at the Robert Koch Institute. His research interests include infectious disease epidemiology and international health.
Acknowledgments
We are grateful to the German Pediatric Surveillance Unit (ESPED), in particular Beate Heinrich for managing the study centers. We acknowledge all contributing medical doctors and clinics for their valuable information and time.
This project was funded by the Robert Koch Institute.
References
- Robert Koch Institute. Report on Influenza epidemiology in Germany, 2009–10 season [in German] [cited 2012 May 2]. http://influenza.rki.de/Saisonberichte/2009.pdf
- Robert Koch-Institute. Influenza-Weekly Report, Germany, 2010 [in German] [cited 2012 May 2]. http://influenza.rki.de/Wochenberichte/2009_2010/2010-31.pdf
- Poggensee G, Gilsdorf A, Buda S, Eckmanns T, Claus H, Altmann D, The first wave of pandemic influenza (H1N1) 2009 in Germany: from initiation to acceleration. BMC Infect Dis. 2010;10:155. DOIPubMedGoogle Scholar
- Wilking H, Buda S, von der Lippe E, Altmann D, Krause G, Eckmanns T, Mortality of 2009 pandemic influenza A(H1N1) in Germany. Euro Surveill. 2010;15:19741.PubMedGoogle Scholar
- Altmann M, Fiebig L, Soyka J, von Kries R, Dehnert M, Haas W. Severe cases of pandemic (H1N1) 2009 in children, Germany. Emerg Infect Dis. 2011;17:186–92. DOIPubMedGoogle Scholar
- World Health Organization. H1N1 in post-pandemic period [cited 2012 May 2]. http://www.who.int/mediacentre/news/statements/2010/h1n1_vpc_20100810/en/index.html
- Morens DM, Taubenberger JK, Harvey HA, Memoli MJ. The 1918 influenza pandemic: lessons for 2009 and the future. Crit Care Med. 2010;38(Suppl):e10–20. DOIPubMedGoogle Scholar
- Miller MA, Viboud C, Balinska M, Simonsen L. The signature features of influenza pandemics–implications for policy. N Engl J Med. 2009;360:2595–8. DOIPubMedGoogle Scholar
- Andreasen V, Viboud C, Simonsen L. Epidemiologic characterization of the 1918 influenza pandemic summer wave in Copenhagen: implications for pandemic control strategies. J Infect Dis. 2008;197:270–8. DOIPubMedGoogle Scholar
- Poulakou G, Souto J, Balcells J, Perez M, Laborda C, Roca O, First influenza season after the 2009 pandemic influenza: characteristics of intensive care unit admissions in adults and children in Vall d'Hebron Hospital. Clin Microbiol Infect. 2012;18:374–80. DOIPubMedGoogle Scholar
- Streng A, Grote V, Liese JG. Severe influenza cases in paediatric intensive care units in Germany during the pre-pandemic seasons 2005 to 2008. BMC Infect Dis. 2011;11:233. DOIPubMedGoogle Scholar
- Cao B, Li XW, Mao Y, Wang J, Lu HZ, Chen YS, Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in China. N Engl J Med. 2009;361:2507–17. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Influenza-associated pediatric deaths—United States, September 2010–August 2011. MMWR Morb Mortal Wkly Rep. 2011;60:1233–8.PubMedGoogle Scholar
- Cox CM, Blanton L, Dhara R, Brammer L, Finelli L. 2009 Pandemic influenza A (H1N1) deaths among children–United States, 2009–2010. Clin Infect Dis. 2011;52(Suppl 1):S69–74. DOIPubMedGoogle Scholar
- Mathews JD, McBryde ES, McVernon J, Pallaghy PK, McCaw JM. Prior immunity helps to explain wave-like behaviour of pandemic influenza in 1918–9. BMC Infect Dis. 2010;10:128. DOIPubMedGoogle Scholar
- Barry JM, Viboud C, Simonsen L. Cross-protection between successive waves of the 1918–1919 influenza pandemic: epidemiological evidence from US Army camps and from Britain. J Infect Dis. 2008;198:1427–34. DOIPubMedGoogle Scholar
- von Kries R, Weiss S, Falkenhorst G, Wirth S, Kaiser P, Huppertz HI, Post-pandemic seroprevalence of pandemic influenza A (H1N1) 2009 infection (swine flu) among children <18 years in Germany. PLoS ONE. 2011;6:e23955. DOIPubMedGoogle Scholar
- Eshima N, Tokumaru O, Hara S, Bacal K, Korematsu S, Tabata M, Sex- and age-related differences in morbidity rates of 2009 pandemic influenza A H1N1 virus of swine origin in Japan. PLoS ONE. 2011;6:e19409. DOIPubMedGoogle Scholar
- Athanasiou M, Baka A, Andreopoulou A, Spala G, Karageorgou K, Kostopoulos L, Influenza surveillance during the post-pandemic influenza 2010/11 season in Greece, 04 October 2010 to 22 May 2011. Euro Surveill. 2011;16:20004.PubMedGoogle Scholar
- Bandaranayake D, Jacobs M, Baker M, Hunt D, Wood T, Bissielo A, The second wave of 2009 pandemic influenza A(H1N1) in New Zealand, January-October 2010. Euro Surveill. 2011;16:19788.PubMedGoogle Scholar
- World Health Organization. Recommended composition of influenza virus vaccines for use in the 2012 southern hemisphere influenza season [cited 2012 May 2]. http://www.who.int/influenza/vaccines/virus/recommendations/2011_09_recommendation.pdf
- Morrison C, Maurtua-Neumann P, Myint MT, Drury SS, Begue RE. Pandemic (H1N1) 2009 outbreak at camp for children with hematologic and oncologic conditions. Emerg Infect Dis. 2011;17:87–9. DOIPubMedGoogle Scholar
- Buda S, Kopke K, Haas W. Epidemiological characteristics of the influenza pandemic (H1N1) 2009 in Germany based on the mandatory notification of cases [in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2010;53:1223–30. DOIPubMedGoogle Scholar
- Mendoza Sánchez MC, Ruiz-Contreras J, Vivanco JL, Fernandez-Carrion F, Baro Fernandez M, Ramos JT, Respiratory virus infections in children with cancer or HIV infection. J Pediatr Hematol Oncol. 2006;28:154–9. DOIPubMedGoogle Scholar
- Spaeder MC, Fackler JC. Hospital-acquired viral infection increases mortality in children with severe viral respiratory infection. Pediatr Crit Care Med. 2011;12:e317–21. DOIPubMedGoogle Scholar
- Liu C, Schwartz BS, Vallabhaneni S, Nixon M, Chin-Hong PV, Miller SA, Pandemic (H1N1) 2009 infection in patients with hematologic malignancy. Emerg Infect Dis. 2010;16:1910–7. DOIPubMedGoogle Scholar
- Brandt C, Rabenau HF, Bornmann S, Gottschalk R, Wicker S. The impact of the 2009 influenza A(H1N1) pandemic on attitudes of healthcare workers toward seasonal influenza vaccination 2010/11. Euro Surveill. 2011;16:19854.PubMedGoogle Scholar
- Böhmer MM, Walter D, Muters S, Krause G, Wichmann O. Seasonal influenza vaccine uptake in Germany 2007/2008 and 2008/2009: results from a national health update survey. Vaccine. 2011;29:4492–8. DOIPubMedGoogle Scholar
- Khouzam RN, Parizianu C, Hafiz AM, Chawla S, Schwartz R. Fulminant myocarditis associated with novel H1N1 influenza A. Heart Lung. 2011;40:566–8. DOIPubMedGoogle Scholar
- Komai T, Nakazawa G, Asai S, Ikari Y. Fatal fulminant myocarditis associated with novel influenza A (H1N1) infection. Eur Heart J. 2011;32:283. DOIPubMedGoogle Scholar
- Randolph AG, Vaughn F, Sullivan R, Rubinson L, Thompson BT, Yoon G, Critically ill children during the 2009–2010 influenza pandemic in the United States. Pediatrics. 2011;128:e1450–8. DOIPubMedGoogle Scholar
- Yung M, Slater A, Festa M, Williams G, Erickson S, Pettila V, Pandemic H1N1 in children requiring intensive care in Australia and New Zealand during winter 2009. Pediatrics. 2011;127:e156–63. DOIPubMedGoogle Scholar
- Kendirli T, Demirkol D, Yildizdacs D, Anil AB, Acsilioglu N, Karapinar B, Critically ill children with pandemic influenza (H1N1) in pediatric intensive care units in Turkey. Pediatr Crit Care Med. 2012;13:e11–7. DOIPubMedGoogle Scholar
- van Zwol A, Witteveen R, Markhorst D, Geukers VG. Clinical features of a Dutch cohort of critically ill children due to the 2009 new influenza A H1N1 pandemic. Clin Pediatr (Phila). 2011;50:69–72. DOIPubMedGoogle Scholar
- Bagdure D, Curtis DJ, Dobyns E, Glode MP, Dominguez SR. Hospitalized children with 2009 pandemic influenza A (H1N1): comparison to seasonal influenza and risk factors for admission to the ICU. PLoS ONE. 2010;5:e15173. DOIPubMedGoogle Scholar
- Heinonen S, Silvennoinen H, Lehtinen P, Vainionpaa R, Vahlberg T, Ziegler T, Early oseltamivir treatment of influenza in children 1–3 years of age: a randomized controlled trial. Clin Infect Dis. 2010;51:887–94. DOIPubMedGoogle Scholar
- Harper SA, Bradley JS, Englund JA, File TM, Gravenstein S, Hayden FG, Seasonal influenza in adults and children–diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis. 2009;48:1003–32. DOIPubMedGoogle Scholar
- German Society for Pediatric Infectious Diseases. Aktualisierte Empfehlung der DGPI zur Diagnostik, Therapie und Prophylaxe der Infektion mit dem Neuen Influenza A/H1N1v-Virus bei Kindern und Jugendlichen. 2009 [cited 2012 May 2]. http://www.dgpi.de/pdf/InflA%20_H1N1v_DGPI-Empfehlungen_09Nov2009.pdf
- German Standing Vaccination Committee (STIKO). Epidemiological Bulletin—vaccination against new Influenza A (H1N1) 2009 [in German] [cited 2012 Aug 15]. http://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2009/Ausgaben/41_09.pdf?__blob=publicationFile
- World Health Organization. Influenza update–06 May 2011 [cited 2011 May 13]. http://www.who.int/influenza/surveillance_monitoring/updates/2011_05_06_GIP_surveillance/en/index.html
Figures
Tables
Cite This ArticleTable of Contents – Volume 18, Number 11—November 2012
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Mathias Altmann, Robert Koch Institute, Department for Infectious Disease Epidemiology, Respiratory Infections Unit, Postfach 65 02 61, 13302 Berlin, Germany
Top