Volume 21, Number 8—August 2015
Research
Response Strategies against Meningitis Epidemics after Elimination of Serogroup A Meningococci, Niger
Figure 3
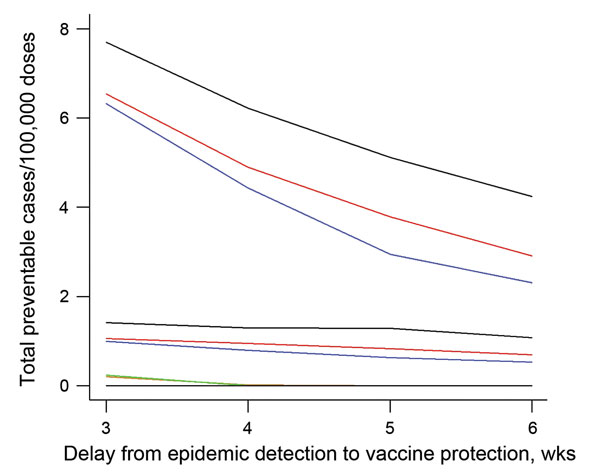
Figure 3. Comparison of preventable meningitis cases per 100,000 vaccine doses, given different surveillance and meningococcal vaccine response strategies, in a situation simulating elimination of Neisseria meningitides serogroup A, Tahoua, Tillabery, and Dosso regions, Niger, 2002–2012. Three, 4, 5, and 6 weeks delay were considered between epidemic detection and effective vaccine protection. The strategies were surveillance and vaccination at health area level (health area–health area, top 3 lines), surveillance at health area level combined with vaccination of the district (health area–district, middle 3 lines), and surveillance and vaccination at district level (district–district, bottom 3 lines). For the health area–health area and health area–district strategies, the black line indicates preventable cases/100,000 vaccine doses at an incidence threshold of 7 cases/100,000 inhabitants; red line, threshold of 10 cases/100,000 inhabitants; and blue line, threshold of 15 cases/100,000 inhabitants. For the district–district strategy, the green line indicates preventable cases/100,000 vaccine doses at an incidence threshold of 4 cases/100,000 inhabitants; orange line, threshold of 2 cases/100,000 inhabitants; and black line, threshold of 7 cases/100,000 inhabitants.