Volume 19, Number 5—May 2013
Research
Changes in Severity of Influenza A(H1N1)pdm09 Infection from Pandemic to First Postpandemic Season, Germany
Cite This Article
Citation for Media
Abstract
We studied risk factors for a severe clinical outcome in hospitalized patients with laboratory-confirmed influenza A(H1N1)pdm09 infection at the University Hospital Heidelberg in the pandemic and first postpandemic seasons. We identified 102 patients in 2009–10 and 76 in 2010–11. The proportion of severely diseased patients dramatically increased from 14% in 2009–10 to 46% in 2010–11 as did the mortality rate (5%–12%). Patients in the first postpandemic season were significantly older (38 vs. 18 years) and more frequently had underlying medical conditions (75% vs. 51%). Overall, 50 patients (28%) had a severe clinical outcome, resulting in 14 deaths. Multivariate analysis showed that older male patients with chronic lung disease were at increased risk for a severe clinical outcome. In summary, the proportion of patients with severe disease and fatal cases increased in the postpandemic season. Therefore, patients with suspected infections should be promptly identified and receive early treatment.
Influenza pandemics have been associated with increased illness and death. Each pandemic is different, and areas of uncertainty always exist when an influenza virus emerges and becomes pandemic. In April 2009, the novel influenza A(H1N1)pdm09 virus emerged in Mexico and then spread rapidly throughout the world (1). Influenza is generally a self-limiting infection with systemic and respiratory symptoms that usually resolve after 3–6 days. Most persons infected with the 2009 influenza A(H1N1)pdm09 virus experienced uncomplicated illness with full recovery within 1 week, even without medical treatment; severe progressive disease developed in only a small subset of patients (2). Primary viral pneumonia was the most common finding in severe cases, but secondary bacterial infections played a role in ≈30% of fatal cases (3). Hospitalized patients were often affected by other medical conditions, such as diabetes and cardiovascular, neurologic and pulmonary diseases (4). Advances in therapy for malignancies, autoimmune disorders, and end-stage organ diseases have led to improved survival, but also to an increase in the number of immunosuppressed patients. These patients are particularly at risk for opportunistic and community-acquired infections, such as respiratory virus infections, resulting in considerable illness and death (5).
Although patients hospitalized with pandemic influenza A(H1N1)pdm09 infection had substantial severe illness, the overall number of deaths was lower than reported in the earliest studies. The overall number of deaths caused by influenza A(H1N1)pdm09 infection was similar to that caused by seasonal influenza and lower than that of previous pandemics (6). The most common cause of death was respiratory failure (7). Other reported causes of death included pneumonia, high fever leading to neurologic sequelae, dehydration from excessive vomiting and diarrhea, and electrolyte imbalance. Severe cases were most frequent in middle-aged patients, who often had coexisting conditions (7). Although to date there seems to be no major difference between the virulence of influenza A(H1N1)pdm09 strains and seasonal influenza (8) strains, a more aggressive course in specific populations, such as in young patients and pregnant women, has been reported (9,10). Further risk factors include obesity, chronic lung disease, chronic heart disease, chronic renal disease, diabetes mellitus, and severe immunosuppression (4,11,12). Contradictory findings have been reported in regard to varying disease severity during the pandemic season. Although some researchers did not observe any differences in disease severity between the first and second pandemic outbreaks in 2009 (13,14), another study showed a 4-fold increase in hospitalization and a 5-fold increase in number of deaths in the second wave (15). However, disease severity of postpandemic seasons has been rarely analyzed.
We performed a retrospective analysis of all patients with laboratory-confirmed influenza A(H1N1)pdm09 virus infection who were hospitalized at the University Hospital Heidelberg, Germany, in the pandemic season 2009–10 and the first postpandemic season 2010–11 to compare the rates of severely diseased patients in both seasons and to identify possible risk factors associated with severe clinical outcome.
Patients and Study Site
We conducted a retrospective cohort study of all patients admitted to the University Hospital Heidelberg, Germany, with laboratory-confirmed influenza A(H1N1)pdm09 infection from May 2009 through April 2011. We defined a case-patient as a hospitalized person with influenza-like illness and influenza A(H1N1)pdm09 virus infection confirmed by real-time PCR. We extracted positive influenza results from our laboratory information system and reviewed the patient charts for clinical and laboratory characteristics as described below. Additionally, we differentiated between pandemic and postpandemic season and severe and nonsevere infections. Severe disease was defined as either admission to the intensive care unit (ICU) or in-hospital death. Microbiologic studies, hospital and ICU admission criteria, and treatment decisions were not standardized but made at the discretion of the attending physicians.
Data Collection
We collected data on demographic characteristics, coexisting conditions, clinical signs and symptoms, biochemical analyses, chest radiograph findings, antiviral and antibacterial therapy, concomitant and secondary bacterial infections as well as outcome, including death. Pneumonia was defined as the presence of a new infiltrate shown on a chest radiograph plus fever (temperature >38°C) and respiratory symptoms. Bacterial infections were diagnosed by means of blood cultures and analysis of sputum or bronchoalveolar lavage specimens. Routine laboratory analyses included C-reactive protein level and leukocyte count.
PCR
Nasopharyngeal samples and bronchoalveolar lavage specimens were collected from the patients and either processed within 2 hours or refrigerated at −20°C. PCR-based detection of influenza A(H1N1)pdm09 and seasonal influenza A and B strains was performed by 1-step real-time reverse transcription PCR (16). Total RNA from respiratory samples was isolated with the QIAamp Viral RNA Mini Kit (QIAGEN, Hilden, Germany), according to the manufacturer’s protocol and reverse transcribed by using random hexamers from the Transcriptor First Strand cDNA Synthesis Kit (Roche, Mannheim, Germany). Reverse transcription PCR analysis was performed with 5.0 μL RNA by using the RNA Virus Master Kit (Roche,) and the LightCycler 480 System (Roche) under the following conditions: 8 min at 50°C; 30 s at 95°C; 50 cycles of 5 s at 95°C, 20 s at 60°C and 1 s at 72°C. The primer pairs were used at a concentration of 10 μM.
Statistical Analysis
To describe the temporal distribution of admitted influenza cases, we aggregated cases by calendar week and compared our data with data from the German surveillance system of mandatory notifiable, laboratory-confirmed influenza cases (17). We summarized demographic and clinical data for time and severity. Frequencies were compared by using χ2 test or Fisher exact test for categorical variables and the Student t test or Mann-Whitney U-test for continuous variables, as appropriate. Identified risk factors with a p value <0.2 in the univariate analysis were included in a multivariate logistic regression model to assess independent association with severity. In a stepwise backward procedure, exposures with p>0.05 were excluded from the model. All comparisons with p<0.05 were considered statistically significant. We used Stata version 11 SE (StataCorp. LP, College Station, TX, USA) for all statistical analyses.
Descriptive Epidemiology
We identified 178 hospitalized patients that fulfilled our case definition and included them in the study group. In the 2009 influenza pandemic season, August 2009 through April 2010, a total of 102 patients with influenza A(H1N1)pdm09 infection were admitted to the Heidelberg University Hospital. In the first postpandemic season (December 2010–March 2011), the number decreased to 76 patients. During the pandemic season, no influenza cases other than influenza A(H1N1)pdm09 infection were observed, whereas in the first postpandemic season, 4 patients received a diagnosis of influenza B virus infection. However, we did not include these influenza B–infected patients in this study.
Epidemic Curve and Age Distribution of Influenza A (H1N1) Case-Patients
Figure 1

Figure 1. . Epidemic curve of influenza A(H1N1)pdm09 virus infections. A) Season 2009–10 and B) season 2010–11. Weeks are indicated; black indicates influenza A(H1N1)pdm09 cases found in the study group at University Hospital...
We charted the temporal distribution of influenza case-patients admitted to the University Hospital Heidelberg by date of first positive laboratory result, compared with influenza cases notified to the German national surveillance system by date of notification (Figure 1). The first observed admission occurred in August 2009 when only sporadic cases of influenza were observed in Germany. The number of admissions increased in October during the first wave with measurable effects of disease at the population level, preceding the usual beginning of the seasonal epidemic by 3 months. The distribution patterns of admissions to Heidelberg University Hospital and notified cases in Germany are similar, both in the pandemic and postpandemic year. In the 2010–11 season, the first cases of influenza were diagnosed in late December in Heidelberg, which is consistent with the usual start of the influenza season.
Figure 2
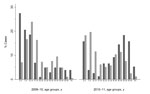
Figure 2. . Age distribution of persons with influenza A(H1N1)pdm09 virus infections, winter 2009–10 and winter 2010–11. Black indicates influenza A(H1N1)pdm09 cases found in the study group at University Hospital Heidelberg; gray indicates...
The distribution of influenza cases among age groups is shown in Figure 2. In the pandemic season >50% of cases from the German national surveillance system were in adolescents (5–19 years of age). In the subsequent season, this pattern shifted to younger children with >50% of cases in patients <14 years of age. The age distribution of patients admitted to the University Hospital of Heidelberg differed from the German national data with higher rates of children <10 years of age in 2009–10 and higher rates in persons >50 years of age in the 2010–11 season.
Comparison of the 2 Seasons
The demographic and clinical characteristics of patients by influenza season are compared in Table 1. In both seasons, the sex distribution was balanced (55% male patients in 2009–10 vs. 47% in 2010-11). However, patients in the first postpandemic season tended to be older (mean age 38 vs. 18 years, p<0.05) than patients in the pandemic season and had a higher proportion of concomitant medical conditions (75% vs. 51%, p<0.05). Furthermore, an increased severity was observed in 2010–11 with a doubled mean duration of hospitalization (13.9 days vs. 7.6 days, p<0.05) and a tripled rate of patients with severe disease (46% vs. 14%, p<0.05). The mortality rate was 12% in 2010–11 compared with 5% in 2009–10 (p = 0.05).
Comparison of Patients with Severe and Nonsevere Disease
Of the 178 patients with influenza A(H1N1)pdm09 infection hospitalized in both seasons, 50 patients (28.1%) had a severe course of infection; of these, 14 died. In univariate analysis, severity of disease was significantly associated with age, presence of pneumonia as well as with a history of an underlying medical condition, in particular, immunosuppression, chronic lung disease, cardiovascular disease, renal impairment, and diabetes (Table 2). In multivariate analysis, 4 independent risk factors for a severe clinical outcome were identified (Table 3): age, male sex, chronic lung disease, and infection in the postpandemic season were significantly associated with severity of disease. The rate of bacterial co-infection increased from 10% to ≈30% in the postpandemic season, but this rate may have been underestimated because microbiologic investigations were not performed routinely for all patients (data not shown).
Demographic and clinical characteristics of influenza patients with a fatal outcome are shown in Table 4. Notably, all 14 case-patients who died had an underlying medical condition; 4 of 14 had multiple myeloma.
Multivariable Analysis of Risk Factors for Disease Severity
Our multivariable logistic regression model identified 4 independent risk factors for severe clinical disease (Table 3). Older, male patients with any chronic lung disease were more affected in the postpandemic season. The other variables mentioned in Table 2 did not reach statistical significance and were therefore not included in our final model.
In our study, the rate of severely diseased patients with influenza A(H1N1)pdm09 virus infection increased 3-fold in the first postpandemic season, resulting in an in-hospital mortality rate of 12% compared with 5% in the pandemic season. Also, the length of hospital stay doubled in the postpandemic season, and the need for mechanical ventilation and ICU admission were significantly higher. We identified older age, male sex, any chronic lung disease, and diagnosis in the postpandemic season as independent risk factors for a severe clinical course of disease. Our study was performed in a retrospective manner without standardized data collection. Information in the medical records can be incomplete, especially for the classification for severe outcome and underlying medical conditions. Therefore, no established scoring system like the pneumonia severity index could be used in classifying severe clinical course.
Influenza A(H1N1)pdm09 virus in the 2009–10 season affected mainly children and young adults in Germany (18). Most hospitalized case-patients in our study group in 2009–10 were young patients, confirming that children and young adults were the age category mostly affected by the pandemic. The low prevalence of older patients in the pandemic season has been attributed to residual immunity against influenza A(H1N1)pdm09 strains in persons born before 1950 (19). Previous studies found that current (20,21) and past pandemics (22) affected mainly younger patients. This finding is in contrast with findings of epidemiologic features of seasonal influenza, for which hospitalizations are more common among persons ≥65 years of age and those <15 years.
The highest increase in seroprevalence between pre- and postpandemic periods was observed among patients 18–29 years of age in Germany (23). In the United Kingdom, population-based evaluation of serologic immunity to the pandemic strain after the pandemic season suggested that susceptibility was lowest in age groups <15 years, with substantial remaining susceptibility in the those 15–44 years (24). Because the remaining susceptibility in children is limited, the probability of extensive illness in this age group with influenza A(H1N1)pdm09 virus in the 2010–11 season was unlikely in the absence of substantial antigenic change in the pandemic virus. Early in the 2010–11 season, high rates of positivity are most marked in those ages 15 to 44 years, the major group contributing to hospital admissions and death (25). This result is in contrast to findings in the 2009–10 pandemic when highest rates of infection in the community were observed in children. The increase in severe courses of infection and requirement for critical care in 2010–11 might reflect the effects of influenza A(H1N1)pdm09 illness in the remaining susceptible adults and risk groups in the population, primarily older patients with coexisting conditions—the historically recognized risk factors for seasonal influenza.
Younger age, chronic coexisting conditions, morbid obesity, and bacterial coinfection have been reported as independent risk factors for severe disease in the pandemic season (3,4). Of hospitalized patients with severe influenza A(H1N1)pdm09 infection, 15%–20% were immunosuppressed in the pandemic season (3,4). These data are in line with a rate of 27% of immunosuppressed patients in our cohort. It might be speculated that hematologic malignancy or treatment of hematologic disorders is an independent risk factor for fatal disease. Studies involving patients with pandemic influenza A(H1N1)pdm09 infection found that although older patients had the lowest estimated incidence rate, they also had the highest case-fatality rate (6). Delayed hospital admission and delayed antiviral therapy have been associated with an unfavorable outcome in the general population and among solid-organ recipients (12). The case-fatality rate increased from 5% to 13% in patients we studied; a lower rate of 3% in the pandemic season had been reported previously (26). Bacterial coinfection is common in case-patients with a fatal outcome (27–29) and has also been observed in our patients who died. Thus, timely administration of antiviral and/or antibacterial drug therapy is indicated in high-risk patients.
The increase of severe and even fatal cases in hospitalized patients with influenza A(H1N1)pdm09 infection in the subsequent season of the pandemic has also been reported by the Novel Influenza A (H1N1) Study Group of the Spanish Network for Research in Infectious Diseases (30) in Spain. Severe clinical courses have been described for patients with underlying conditions, pregnant women, and obese patients (4,10). In 2009, this study group observed similar rates of severe disease (31) to our observations, namely, 28% with pneumonia and 15% with severe disease. Molecular characterization of influenza A(H1N1)pdm09 viruses circulating in 2010 revealed only a minor genetic drift compared with early isolates from 2009 (25), which most likely cannot be attributed for the change in clinical outcome.
In conclusion, we found notable epidemiologic changes and an increased severity of influenza A(H1N1)pdm09 infections in the first postpandemic influenza season. These findings reinforce the need to identify and protect groups at highest risk for adverse outcomes.
Dr Lehners is a resident physician in the Department of Hematology and Oncology at the University of Heidelberg, Germany. Her main research interests are pathogenesis and clinical management of infectious diseases in the immunocompromised host.
Acknowledgment
We thank W. Alle for help with laboratory database analysis.
References
- Fraser C, Donnelly CA, Cauchemez S, Hanage WP, Van Kerkhove MD, Hollingsworth TD, Pandemic potential of a strain of influenza A (H1N1): early findings. Science. 2009;324:1557–61 and. DOIPubMedGoogle Scholar
- Cullen G, Martin J, O’Donnell J, Boland M, Canny M, Keane E, Surveillance of the first 205 confirmed hospitalised cases of pandemic H1N1 influenza in Ireland, 28 April–3 October 2009. Euro Surveill. 2009;14: pii: 19389.
- CDC. Bacterial coinfections in lung tissue specimens from fatal cases of 2009 pandemic influenza A (H1N1)—United States, May–August 2009. MMWR Morb Mortal Wkly Rep. 2009;58:1071–4 .PubMedGoogle Scholar
- Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, Hospitalized patients with 2009 H1N1 influenza in the United States, April–June 2009. N Engl J Med. 2009;361:1935–44. DOIPubMedGoogle Scholar
- Ljungman P, Andersson J, Aschan J, Barkholt L, Ehrnst A, Johansson M, Influenza A in immunocompromised patients. Clin Infect Dis. 1993;17:244–7. DOIPubMedGoogle Scholar
- Donaldson LJ, Rutter PD, Ellis BM, Greaves FE, Mytton OT, Pebody RG, Mortality from pandemic A/H1N1 2009 influenza in England: public health surveillance study. BMJ. 2009;339:b5213. DOIPubMedGoogle Scholar
- Estenssoro E, Rios FG, Apezteguia C, Reina R, Neira J, Ceraso DH, Pandemic 2009 influenza A in Argentina: a study of 337 patients on mechanical ventilation. Am J Respir Crit Care Med. 2010;182:41–8. DOIPubMedGoogle Scholar
- 8. York I, Donis RO. The 2009 pandemic influenza virus: where did it come from, where is it now, and where is it going? [Epub ahead of print] Curr Top Microbiol Immunol. 2012;•••:26.
- Chowell G, Bertozzi SM, Colchero MA, Lopez-Gatell H, Alpuche-Aranda C, Hernandez M, Severe respiratory disease concurrent with the circulation of H1N1 influenza. N Engl J Med. 2009;361:674–9. DOIPubMedGoogle Scholar
- Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, Biggerstaff MS, H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009;374:451–8. DOIPubMedGoogle Scholar
- Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic. (H1N1) 2009 Influenza. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. 2010;362:1708–19 . DOIPubMedGoogle Scholar
- Kumar D, Michaels MG, Morris MI, Green M, Avery RK, Liu C, Outcomes from pandemic influenza A H1N1 infection in recipients of solid-organ transplants: a multicentre cohort study. Lancet Infect Dis. 2010;10:521–6 . DOIPubMedGoogle Scholar
- Ramakrishna K, Peter JV, Karthik G, Abraham AM, Surekha V, Karthik R, Influenza A (H1N1) 2009 pandemic: was there a difference in the two waves in patients requiring admission to the intensive-care unit? Clin Microbiol Infect. 2011;17:1355–8 .PubMedGoogle Scholar
- Altmann M, Fiebig L, Buda S, von Kries R, Dehnert M, Haas W. Unchanged severity of influenza A(H1N1)pdm09 infection in children during first postpandemic season. Emerg Infect Dis. 2012;18:1755–62 . DOIPubMedGoogle Scholar
- Truelove SA, Chitnis AS, Heffernan RT, Karon AE, Haupt TE, Davis JP. Comparison of patients hospitalized with pandemic 2009 influenza A (H1N1) virus infection during the first two pandemic waves in Wisconsin. J Infect Dis. 2011;203:828–37. DOIPubMedGoogle Scholar
- Panning M, Eickmann M, Landt O, Monazahian M, Olschlager S, Baumgarte S, Detection of influenza A(H1N1)v virus by real-time RT-PCR. Euro Surveill. 2009;14:19329 .PubMedGoogle Scholar
- Robert-Koch-Institute. SurvStat [cited 2012 Sep 17]. http://www3.rki.de/SurvStat.
- Poggensee G, Gilsdorf A, Buda S, Eckmanns T, Claus H, Altmann D, The first wave of pandemic influenza (H1N1) 2009 in Germany: from initiation to acceleration. BMC Infect Dis. 2010;10:155. DOIPubMedGoogle Scholar
- Pérez-Trallero E, Pineiro L, Vicente D, Montes M, Cilla G. Residual immunity in older people against the influenza A(H1N1)–recent experience in northern Spain. Euro Surveill. 2009;14:19344 .PubMedGoogle Scholar
- Miller RR III, Markewitz BA, Rolfs RT, Brown SM, Dascomb KK, Grissom CK, Clinical findings and demographic factors associated with ICU admission in Utah due to novel 2009 influenza A(H1N1) infection. Chest. 2010;137:752–8. DOIPubMedGoogle Scholar
- Viasus D, Pano-Pardo JR, Pachon J, Campins A, Lopez-Medrano F, Villoslada A, Factors associated with severe disease in hospitalized adults with pandemic (H1N1) 2009 in Spain. Clin Microbiol Infect. 2011;17:738–46. DOIPubMedGoogle Scholar
- Erkoreka A. The Spanish influenza pandemic in occidental Europe (1918–1920) and victim age. Influenza Other Respi Viruses. 2010;4:81–9. DOIPubMedGoogle Scholar
- Dudareva S, Schweiger B, Thamm M, Hohle M, Stark K, Krause G, Prevalence of antibodies to 2009 pandemic influenza A (H1N1) virus in German adult population in pre- and post-pandemic period. PLoS ONE. 2011;6:e21340. DOIPubMedGoogle Scholar
- Hardelid P, Andrews NJ, Hoschler K, Stanford E, Baguelin M, Waight PA, Assessment of baseline age-specific antibody prevalence and incidence of infection to novel influenza A/H1N1 2009. Health Technol Assess. 2010;14:115–92 .PubMedGoogle Scholar
- Ellis J, Galiano M, Pebody R, Lackenby A, Thompson C, Bermingham A, Virological analysis of fatal influenza cases in the United Kingdom during the early wave of influenza in winter 2010/11. Euro Surveill. 2011;16:19760 .PubMedGoogle Scholar
- Bassetti M, Parisini A, Calzi A, Pallavicini FM, Cassola G, Artioli S, Risk factors for severe complications of the novel influenza A (H1N1): analysis of patients hospitalized in Italy. Clin Microbiol Infect. 2011;17:247–50. DOIPubMedGoogle Scholar
- Cordero E, Aydillo T, Farinas MC, Pano-Pardo JR, Pachon J, Viasus D, Immunosuppressed patients with pandemic influenza A 2009 (H1N1) virus infection. Eur J Clin Microbiol Infect Dis. 2012;31:547–56. DOIPubMedGoogle Scholar
- Morens DM, Taubenberger JK, Fauci AS. Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. J Infect Dis. 2008;198:962–70. DOIPubMedGoogle Scholar
- Rihani R, Hayajneh W, Sultan I, Ghatasheh L, Abdel-Rahman F, Hussein N, Infections with the 2009 H1N1 influenza virus among hematopoietic SCT recipients: a single center experience. Bone Marrow Transplant. 2011;46:1430–6. DOIPubMedGoogle Scholar
- Viasus D, Cordero E, Rodriguez-Bano J, Oteo JA, Fernandez-Navarro A, Ortega L, Changes in epidemiology, clinical features and severity of influenza A (H1N1) 2009 pneumonia in the first post-pandemic influenza season. Clin Microbiol Infect. 2012;18:E55–62. DOIPubMedGoogle Scholar
- Viasus D, Pano-Pardo JR, Cordero E, Campins A, Lopez-Medrano F, Villoslada A, Effect of immunomodulatory therapies in patients with pandemic influenza A (H1N1) 2009 complicated by pneumonia. J Infect. 2011;62:193–9. DOIPubMedGoogle Scholar
Figures
Tables
Cite This Article1These authors contributed equally to this article.
Table of Contents – Volume 19, Number 5—May 2013
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Paul Schnitzler, Department of Infectious Diseases, Virology, Im Neuenheimer Feld 324 69120, Heidelberg, Germany
Top