Volume 21, Number 10—October 2015
Research
Possible Role of Rickettsia felis in Acute Febrile Illness among Children in Gabon
Cite This Article
Citation for Media
Abstract
Rickettsia felis has been reported to be a cause of fever in sub-Saharan Africa, but this association has been poorly evaluated in Gabon. We assessed the prevalence of this bacterium among children <15 years of age in 4 areas of Gabon; the locations were in urban, semiurban, and rural areas. DNA samples from 410 febrile children and 60 afebrile children were analyzed by quantitative PCR. Overall, the prevalence of R. felis among febrile and afebrile children was 10.2% (42/410 children) and 3.3% (2/60 children), respectively. Prevalence differed among febrile children living in areas that are urban (Franceville, 1.3% [1/77]), semiurban (Koulamoutou, 2.1% [3/141]), and rural (Lastourville, 11.2% [15/134]; Fougamou, 39.7% [23/58]). Furthermore, in a rural area (Fougamou), R. felis was significantly more prevalent in febrile (39.7% [23/58]) than afebrile children (5.0% [1/20]). Additional studies are needed to better understand the pathogenic role of R. felis in this part of the world.
Over the past decade, reported cases of malaria and associated deaths have declined in Africa (1). This decrease has led to a search for other causes of fever in Africa, where unexplained febrile illnesses are one of the major health problems. In some sub-Saharan Africa countries, malaria treatments are still administered without a biologic diagnosis. For example, an assessment of complicated malaria and other severe febrile illness cases in a pediatric ward in Libreville, Gabon, showed that 43.5% of the children who received an antimalarial treatment had microscopy test results negative for malaria (2).
Other studies have shown that, in addition to malaria, other bacterial infections are a major cause of fever in Africa (3–6). Staphylococcus aureus, Streptococcus pneumoniae, nontyphoidal Salmonella spp., Klebsiella pneumoniae, and Escherichia coli are the bacteria most often detected in sub-Saharan Africa by the culture method (7,8). The use of molecular tools has enabled the identification of the following fastidious bacteria as a cause of unexplained fevers in Africa: Rickettsia spp., including R. felis (3–5,9); Coxiella burnetii (10); Tropheryma whipplei (11); and Borrelia spp. (12,13). However, the epidemiology of many fastidious bacteria, such as R. felis, remains poorly understood. In rural areas of Senegal, the prevalence of R. felis was generally higher (7%–24%) than that in urban areas of sub-Saharan African, such as Franceville, Gabon (10%) (14).
R. felis is a gram-negative bacterium belonging to the spotted fever group of Rickettsia spp. In Gabon, the bacterium has been reported in arthropods, including Ctenocephalides felis cat fleas (15) and Aedes albopictus mosquitoes (16), and in humans (14). Similar to many African countries, Gabon has a strong disparity between health care in urban and rural areas; in rural areas, little is known about the epidemiology of infectious diseases. The aim of our study was to evaluate the prevalence of R. felis infection among febrile and afebrile children in rural and urban areas of Gabon and the possible role of R. felis in acute febrile illness.
Study Area
Figure 1

Figure 1. Four rural (Fougamou and Lastourville), semiurban (Koulamoutou), and urban (Franceville) locations in Gabon where children <15 years of age were tested for Rickettsia felis infection, April 2013–January 2014. Percentages in parentheses...
Gabon is a central African country located on the equator along the Atlantic Coast (Figure 1). The country has a low coastal plain and hilly inland areas and savannas to the east and south; 80% of Gabon is covered by forest. The tropical climate is hot and humid, and the seasons alternate in precipitation and length: short dry season, long rainy season, long dry season, short rainy season.
Study Design and Participants
Patients were recruited at 4 health centers (Figure 1) located in 3 Gabon provinces. One center, the Regional Hospital Center Amissa Bongo of Franceville, is in an urban area of Haut-Ogooué Province. Two centers, the Regional Hospital Center Paul Moukambi of Koulamoutou and the Medical Center of Lastourville, are in semiurban and rural areas, respectively, of Ogooué Lolo Province. The fourth center, the Medical Research Unit of Ngounie in Fougamou, is in a rural area of Ngounié Province.
The National Ethics Committee of Gabon approved this prospective study (no. 0023/2013/SG/CNE). Written informed consent forms and questionnaires were completed by parents or legal guardians upon a child’s enrollment in the study.
During April 2013–January 2014, a total of 525 children <15 years of age were recruited for the study; 465 of the children were febrile (axillary temperature >37.5°C), and 60 were afebrile (controls). Febrile children were recruited from the pediatric outpatient clinics at the 4 health care centers. The control group was recruited from children who had accompanied their sick parents to the health care centers. Children in the control group had to be free of fever for at least 1 week before study inclusion.
Sample Collection and Molecular Analysis
Molecular analyses were performed on DNA extracts from blood samples from each child; blood smears, serologic testing, and culture were not done. After a child’s parent or legal guardian was interviewed, a blood sample was collected into an EDTA tube. World Health Organization guidelines for blood collection were followed, including guidelines for hand hygiene, use of sterile tubes, and skin disinfection with 70% alcohol. The International Center of Medical Research of Franceville, which has a well-trained staff with expertise in infectious diseases, performed DNA extraction by using the E.Z.N.A. Blood DNA Maxi Kit (Omega Bio-tek, Norcross, GA, USA) according to the manufacturer’s protocol (17). A total of 150 μL of DNA extract was obtained from each sample. The extracts were stored at −20°C before being sent on ice to URMITE (Unité de Recherche sur les Maladies Infectieuses et Tropicales, Marseille, France) for molecular analyses.
Specific quantitative PCR (qPCR) was performed by using a CFX96 Touch Real-Time PCR Detection System (Bio-Rad Laboratories, Marnes-la-Coquette, France). qPCR Master Mix (Eurogentec, Liege, Belgium) was prepared according to the manufacturer’s instructions; for each reaction, 15 μL of Master Mix was added to 5 μL of DNA. The quality of extracted DNA and the lack of PCR inhibitors were systematically checked by targeting a housekeeping gene, human β-actin (14). Positive (R. felis DNA) and negative (mix alone) controls were also systematically used for each PCR assay. All samples were screened by Rickettsia spp.–specific qPCR targeting the gltA gene and by R. felis–specific qPCR targeting the bioB, orfB, and vapB1 genes (14) (Table 1). Samples positive for at least 2 genes were considered positive.
Statistical Analysis
Data were analyzed by using Epi Info software version 7.0.8.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA). Mantel-Haenszel χ2 and Fisher exact tests were used to compare the prevalence between groups (i.e., febrile and afebrile children), seasons, and geographic areas and by the participants’ sex and age. A 2-tailed p value <0.05 was considered statistically significant.
Recruitment
A total of 465 febrile children were recruited from Franceville (n = 80), Koulamoutou (n = 167), Lastourville (n = 155), and Fougamou (n = 63) (Table 2). However, 55 of these children were excluded from the statistical analysis because their sex and age data were unavailable; 3 of the excluded children were from Franceville, 26 from Koulamoutou, 21 from Lastourville, and 2 from Fougamou. Of the 410 children included in the statistical analysis, 52.7% (216/410) were recruited during a rainy season, and 47.3% (194/410) were recruited during a dry season. A total of 60 afebrile children were recruited and enrolled in parallel from Franceville (n = 24), Fougamou (n = 20), and Lastourville (n = 16); no afebrile children were enrolled from Koulamoutou. The 410 febrile patients included in the statistical analysis consisted of 212 boys and 198 girls (sex ratio 1.07).
R. felis in Febrile and Afebrile Children in Gabon
Figure 2
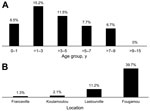
Figure 2. Prevalence of Rickettsia felis infection among febrile children <15 years of age in Gabon, April 2013–January 2014. A) Prevalence by age group. B) Prevalence by location.
R. felis DNA was detected in 42 (10.2%) of 410 analyzed samples from febrile children (Table 3). The bacterium was detected significantly more frequently during the rainy season (15.3% [33/216 samples]) than the dry season (4.6% [9/194 samples]; p<0.001). The prevalence among boys (10.8% [23/212]) and girls (9.6% [19/198]) did not differ significantly (p = 0.74). Among febrile children, R. felis prevalence varied by age group: 8.5% (11/129 children) among children 0–1 year of age, 15.2% (16/105) among children >1– 3 years of age, 11.5% (10/87) children >3–5 years of age, 7.7% (3/39) among children >5–7 years of age, 6.7% (2/30) among children >7–9 years of age, and 0 (0/20) among children >9–15 years of age (Figure 2, panel A). The prevalence of R. felis among febrile children did not differ substantially by age, but the prevalence did increase progressively from Franceville (1.3% [1/77]) to Koulamoutou (2.1% [3/141]) to Lastourville (11.2% [15/134]) to Fougamou (39.7% [23/58]); however, no adjustments were made when testing these pairs (Figure 2, panel B). The prevalence was statistically lower in Franceville than in Lastourville (odds ratio [OR] 0.1, 95% CI 2.5 × 10−3–0.7; p = 0.006), in Franceville than in Fougamou (OR 0.02, 95% CI 5 × 10−4–0.1, p<0.001), in Koulamoutou than in Lastourville (OR 0.17, 95% CI 0.03–0.63; p = 0.002), in Koulamoutou than in Fougamou (OR 0.03, 95% CI 6 × 10−3–0.12; p<0.001), and in Lastourville than in Fougamou (OR 0.19, 95% CI 0.08–0.43; p<0.001). Overall, the prevalence of R. felis among febrile children was significantly higher in the rural areas (Lastourville and Fougamou; 19.8% [38/192 children]) than in the urban area (Franceville; 1.3% [1/77 children]; p<0.001). Among the 60 afebrile children, only 2 (3.3%; both girls) were positive for R. felis; the girls were 1 and 3 years of age and were from Fougamou and Franceville, respectively. In all, R. felis DNA was detected in 10.2% (42/410) of febrile children and in 3.3% (2/60) of afebrile children; this difference was not significant (p = 0.09).
R. felis at Each Sampling Location
Fougamou, Ngounié Province
R. felis DNA was detected in 23 (39.7%) of 58 febrile children at this rural location (Table 3; Figure 2). Prevalence during the rainy season (48.7% [19/39 children]) was higher than that during the dry season (21.1% [4/19 children]; p = 0.05). R. felis prevalence among boys (50% [15/30]) and girls (28.6% [8/28]) did not differ significantly (p = 0.11). R. felis prevalence also did not differ significantly by age, even though prevalence was higher among 1- to 3-year-old children (Table 3). Overall, R. felis DNA was detected significantly more frequently in febrile (39.7% [23/58]) than afebrile (5.0% [1/20]) children (p = 0.004).
Lastourville, Ogooué Lolo Province
R. felis DNA was detected in 15 (11.2%) of 134 febrile children in this rural location (Table 3; Figure 2). R. felis prevalence during the rainy season (15.8% [12/76 children]) was higher than that during the dry season (5.2% [3/58 children]), but the difference was not statistically significant (p = 0.05). Prevalence among boys (7.6% [6/79]) and girls (16.4% [9/55]) did not differ significantly (p = 0.17). Prevalence also did not differ significantly by age (Table 3). R. felis DNA was detected in 15 (11.2%) of 134 febrile children and in 0 of 16 afebrile children; this difference was not statistically significant (p = 0.3).
Koulamoutou, Ogooué Lolo Province
R. felis DNA was detected in 3 (2.1%) of 141 febrile children in this semiurban location (Table 3; Figure 2). Prevalence during the rainy season (2.9% [2/68 children]) was higher than that during the dry season (1.4 [1/73 children]; p = 0.6). R. felis DNA was detected in 1 (1.6%) of 63 boys and in 2 (2.6%) of 78 girls (p<1); 2 of these children were 4 years of age, and 1 was 5 years of age. As stated above, no afebrile children were enrolled from Koulamoutou.
Franceville, Haut-Ogooué Province
R. felis DNA was detected in 1 (1.3%) of 77 febrile children and in 1 (4.2%) of 24 afebrile children (p = 0.3) in this urban area (Table 3; Figure 2). The infected febrile child was a 2-year-old boy, and the infected afebrile child was a 3-year-old girl; both children became infected during the dry season.
The lack of molecular tools in many health centers in countries in sub-Saharan Africa limits the management of all febrile illnesses in these areas. In this study, we used molecular tools (PCR assays) to assess the prevalence of R. felis in blood specimens from febrile and afebrile children from rural, semiurban, and urban areas of Gabon. One of the most frequent pitfalls of PCR assays is the contamination of samples, which can occur any time during or after collection of the samples, including during their use in the laboratory. Over the years, the URMITE laboratory has developed strategies and applied rigorous procedures to prevent and detect contamination (18–21). For example, we require that 2 different PCR assays show positive results before we conclude that a sample is positive (21).
In this study, we used a Rickettsia spp.–specific qPCR targeting the highly conservative gltA gene and an R. felis–specific qPCR targeting the bioB, orfB, and vapB1 genes. The Rickettsia spp.–specific assay can amplify almost all Rickettsia spp., including R. conorii and R. rickettsii, but it is less sensitive than the R. felis–specific assay. When a sample in our study was positive by the Rickettsia spp.–specific qPCR, it was also positive by the R. felis qPCR. Several samples had positive results for only 2 of the 3 genes targeted by the R. felis–specific qPCR. This discrepancy might be explained by possible genetic diversity of the R. felis strains. The 3 genes used for the R. felis–specific assay are not all conservative, so it is possible that some strains have a certain degree of genetic diversity that may occasionally cause false-negative PCR results. Our results were also systematically validated by using rigorous criteria. To check the quality of each PCR run, we used negative controls (i.e., PCR mix without template) with every tenth sample, and we used 2 positive controls (R. felis DNA) per run. In addition, we required that all negative and positive controls be systematically correct (i.e., negative and positive, respectively) before validating each PCR run, and a sample was not considered R. felis–positive unless confirmed by at least 2 of the 4 sequences of targeted DNA. Thus, we consider our results to be valid. The fact that R. felis DNA has not been detected in samples (from febrile patients in France and Tunisia) previously analyzed in our laboratory (14) provides further support of our team’s ability to prevent and detect contamination during PCR runs. Furthermore, it has been reported that the prevalence of R. felis is low in northern Africa countries (France, Algeria, Morocco, Tunisia) and increases in southern Africa countries (Mali, Senegal, Gabon) (14).
Consistent with our previous findings from Franceville in Haut-Ogooué Province (14), our findings from this study confirmed the presence of R. felis bacteremia in febrile children in Gabon and showed that the prevalence of infection was higher in rural than urban and semiurban areas. This fastidious bacterium was previously found in arthropods in Franceville (15), including the cat flea, C. felis. The bacterium was also detected in A. albopictus mosquitoes in Libreville in Estuaire Province (16). Data from our study also confirm the presence of R. felis in children in Ogooué lolo and Ngounié Provinces. Therefore, R. felis is widespread in Gabon, and its prevalence should be assessed in other areas of the country.
Common microorganisms involved in bacteremia (S. aureus, Streptococcus pyogenes, E. coli, K. pneumoniae, Salmonella spp., and S. pneumoniae) were previously assessed in Gabon by using standard culture methods (8), but the prevalence of fastidious bacteria, which are mainly detected by using molecular techniques, was not studied. There is a need to include these sensitive methods in diagnostic determinations. Our findings, plus those from studies in Senegal (14,22), Mali (14), Kenya (5), Ethiopia (23,24), Cameroon (25), Democratic Republic of the Congo (26,27), Ivory Coast (Côte d’Ivoire) (6), and Zimbabwe (28), show that R. felis is widespread in sub-Saharan Africa countries (29). However, its prevalence changes according to the season, year, area (rural, urban, and semiurban), country, and age of those infected.
A comparison of our findings with previously reported data showed that R. felis prevalence among febrile children in Franceville decreased from 10% in 2012 (14) to 1.3% in 2014. In addition, the variation in the R. felis prevalence between urban (1.3%) and rural (39.7%) areas of Gabon showed that R. felis is unequally distributed in the country. Differences in the prevalence of a possible vector or reservoir, or both, and disparate health care–associated conditions, including environmental conditions, poverty, and the availability and quality of health care facilities, between rural and urban areas may influence the distribution of R. felis in Gabon; however, these factors have not been determined. An increased prevalence of R. felis was observed during the rainy season. This same finding was described in Senegal, where the prevalence of infection in the rural areas was 24 times higher than that in urban areas of Algeria (14). Together, the finding suggests that R. felis is more prevalent in rural areas and during the rainy season in sub-Saharan Africa.
R. felis was previously found in C. felis fleas from a pet monkey in Gabon, but the data concerned only 1 region, Franceville (15). R. felis has been reported to be absent from C. felis fleas in rural areas of Senegal, where R. felis is common (30). The factors explaining the spread of R. felis in Gabon should be evaluated in further studies. Although R. felis is widespread in Africa and unequally distributed in Gabon and Senegal (14), its prevalence varies by country: 15.0% in Senegal (14), 3.0% in Mali (14), and 7.2% in Kenya (5). In our study, R. felis was mainly detected in young febrile children <5 years of age (primarily in those 1–3 years of age). In a rural area of Senegal (Dielmo and Ndiop), the incidence of R. felis infection has also been reported to be higher (reaching 36%) among febrile children 1–3 years of age, but the incidence was lower (0.1%) in persons >15 years of age (14). It has been reported that the seroprevalence of R. felis increases with age in areas where the bacterium is endemic (5). This increase is probably due to exposure to the bacterium during the course of a lifetime, leading to protection by a progressive development of immunity against this bacterium in adults.
Most of the fever-associated studies conducted in Africa failed to use a control group of afebrile persons. Consequently, when a pathogen was detected in febrile patients, it was systematically and automatically considered as the cause of fever (7). In some cases, we have also observed a mistake in methodology: data comparisons were performed between samples from afebrile persons in an occidental area and from febrile persons in Africa (31). The epidemiology of microorganisms depends on the studied areas, and the positive predictive value of a disease depends on its symptoms and epidemiology. For example, Plasmodium falciparum, the primary agent of malaria, is commonly detected in blood specimens from apparently healthy, afebrile persons in Sub-Saharan Africa; prevalence can reach 20% in Ethiopia and 32% in Senegal (32,33). Respiratory viruses, including influenza virus, have also been found in 12% of nasopharyngeal samples of asymptomatic Hajj pilgrims (34). More recently in Tanzania, the prevalence of S. pneumoniae DNA was less frequently detected in febrile (5.1%) than afebrile (6.3%) persons (35). Thus, these examples show that even well-known pathogens may be detected in blood or respiratory secretions of afebrile persons. The inclusion of control groups of participants in studies is indispensable to a better understanding of infectious diseases; the use of controls has shown the existence of carriers of well-known pathogens, emphasizing that it is not easy to interpret data about the potential pathogenic role of a microorganism. The finding of R. felis in febrile versus afebrile persons is not well characterized. The overall prevalence of R. felis in Gabon was higher in febrile (10.2%) than afebrile (3.3%) children, but the difference was not statistically significant (p = 0.09). Of more interest, in rural Fougamou, the difference in prevalence was significantly higher in similarly aged children with and without fever (39.7% vs. 5.0%, respectively; p = 0.004). Therefore, the presence of R. felis in febrile and afebrile persons should not exclude that this bacterium is a cause of fever in sub-Saharan Africa.
In 2010, independent research teams detected R. felis in blood specimens from febrile patients in 2 different areas of Africa (eastern and western) (3,4). In other studies, these teams confirmed and extended the preliminary data: 1 team showed that the presence of R. felis was 2.2 times higher in blood specimens from febrile persons compared with afebrile persons in Kenya (5), and the other team showed that the prevalence of R. felis was significantly higher in febrile (15.0%) than afebrile (4.0%) persons in Senegal (14). In Senegal, an 8-month-old febrile girl was cured of R. felis infection after treatment with doxycycline (36). The presence of R. felis has also been observed in blood specimens from febrile patients in Asia (37). The higher prevalence of R. felis among febrile persons compared with healthy persons in our study led us to suspect that this microorganism plays the role of pathogen. However, the presence of the microorganism may be a cofactor or the cause of a previous event not yet determined. Another hypothesis would be that blood specimens may be contaminated by surface bacteria, including R. felis, which has been detected on the skin of healthy persons in Senegal (38).
In summary, the R. felis bacterium is widespread in Gabon, but it primarily occurs in rural areas and is most prominent during the rainy season. R. felis is also more prevalent among febrile than afebrile children in rural areas of Gabon. More studies will help to better understand the pathogenic role of R. felis in this part of the world.
Mr. Mourembou, a PhD student in infectious diseases, works in the Unit of Research on Emergent Infectious and Tropical Diseases in Marseille, France. His main research interest is fever of unknown origin in Gabon.
Acknowledgments
We thank all persons who participated in the study.
This study was funded by the Institut Hospitalo-Universitaire Méditerranée Infection.
References
- D’Acremont V, Lengeler C, Genton B. Reduction in the proportion of fevers associated with Plasmodium falciparum parasitaemia in Africa: a systematic review. Malar J. 2010;9:240 . DOIPubMedGoogle Scholar
- Bouyou-Akotet MK, Mawili-Mboumba DP, Kendjo E, Eyang Ekouma A, Abdou Raouf O, Engohang Allogho E, Complicated malaria and other severe febrile illness in a pediatric ward in Libreville, Gabon. BMC Infect Dis. 2012;12:216 . DOIPubMedGoogle Scholar
- Socolovschi C, Mediannikov O, Sokhna C, Tall A, Diatta G, Bassene H, Rickettsia felis–associated uneruptive fever, Senegal. Emerg Infect Dis. 2010;16:1140–2. DOIPubMedGoogle Scholar
- Richards AL, Jiang J, Omulo S, Dare R, Abdirahman K, Ali A, Human infection with Rickettsia felis, Kenya. Emerg Infect Dis. 2010;16:1081–6. DOIPubMedGoogle Scholar
- Maina AN, Knobel DL, Jiang J, Halliday J, Feikin DR, Cleaveland S, Rickettsia felis infection in febrile patients, western Kenya, 2007–2010. Emerg Infect Dis. 2012;18:328–31 . DOIPubMedGoogle Scholar
- Berrelha J, Briolant S, Muller F, Rolain JM, Marie JL, Pagés F, Rickettsia felis and Rickettsia massiliae in Ivory Coast, Africa. Clin Microbiol Infect. 2009;15(Suppl 2):251–2. DOIPubMedGoogle Scholar
- Reddy EA, Shaw AV, Crump JA. Community-acquired bloodstream infections in Africa: a systematic review and meta-analysis. Lancet Infect Dis. 2010;10:417–32 . DOIPubMedGoogle Scholar
- Alabi AS, Frielinghaus L, Kaba H, Kösters K, Huson MA, Kahl BC, Retrospective analysis of antimicrobial resistance and bacterial spectrum of infection in Gabon, Central Africa. BMC Infect Dis. 2013;13:455. DOIPubMedGoogle Scholar
- Sokhna C, Mediannikov O, Fenollar F, Bassene H, Diatta G, Tall A, Point-of-care laboratory of pathogen diagnosis in rural Senegal. PLoS Negl Trop Dis 2013;7:e1999.
- Mediannikov O, Fenollar F, Socolovschi C, Diatta G, Bassene H, Molez JF, Coxiella burnetii in humans and ticks in rural Senegal. PLoS Negl Trop Dis. 2010;4:e654. DOIPubMedGoogle Scholar
- Fenollar F, Mediannikov O, Socolovschi C, Bassene H, Diatta G, Richet H, Tropheryma whipplei bacteremia during fever in rural West Africa. Clin Infect Dis. 2010;51:515–21 . DOIPubMedGoogle Scholar
- Parola P, Diatta G, Socolovschi C, Mediannikov O, Tall A, Bassene H, Tick-borne relapsing fever borreliosis, rural Senegal. Emerg Infect Dis. 2011;17:883–5. DOIPubMedGoogle Scholar
- Elbir H, Raoult D, Drancourt M. Relapsing fever borreliae in Africa. Am J Trop Med Hyg. 2013;89:288–92. DOIPubMedGoogle Scholar
- Mediannikov O, Socolovschi C, Edouard S, Fenollar F, Mouffok N, Bassene H, Common epidemiology of Rickettsia felis infection and malaria, Africa. Emerg Infect Dis. 2013;19:1775–83. DOIPubMedGoogle Scholar
- Rolain JM, Bourry O, Davoust B, Raoult D. Bartonella quintana and Rickettsia felis in Gabon. Emerg Infect Dis. 2005;11:1742–4.PubMedGoogle Scholar
- Socolovschi C, Pages F, Raoult D. Rickettsia felis in Aedes albopictus mosquitoes, Libreville, Gabon. Emerg Infect Dis. 2012;18:1687–9. DOIPubMedGoogle Scholar
- Lekana-Douki JB, Pontarollo J, Zatra R, Toure-Ndouo FS. Malaria in Gabon: results of a clinical and laboratory study at the Chinese–Gabonese Friendship Hospital of Franceville. Sante. 2011;21:193–8 .PubMedGoogle Scholar
- Morel AS, Dubourg G, Prudent E, Edouard S, Gouriet F, Casalta JP, Complementarity between targeted real-time specific PCR and conventional broad-range 16S rDNA PCR in the syndrome-driven diagnosis of infectious diseases. Eur J Clin Microbiol Infect Dis. 2015;34:561–70. DOIPubMedGoogle Scholar
- Mediannikov O, Fenollar F. Looking in ticks for human bacterial pathogens. Microb Pathog. 2014;77:142–8. DOIPubMedGoogle Scholar
- Fenollar F, Raoult D. Molecular genetic methods for the diagnosis of fastidious microorganisms. APMIS. 2004;112:785–807. DOIPubMedGoogle Scholar
- Lévy PY, Fenollar F. The role of molecular diagnostics in implant-associated bone and joint infection. Clin Microbiol Infect. 2012;18:1168–75. DOIPubMedGoogle Scholar
- Mediannikov O, Diatta G, Fenollar F, Sokhna C, Trape JF, Raoult D. Tick-borne rickettsioses, neglected emerging diseases in rural Senegal. PLoS Negl Trop Dis. 2010;4:e821. DOIPubMedGoogle Scholar
- Kumsa B, Parola P, Raoult D, Socolovschi C. Molecular detection of Rickettsia felis and Bartonella henselae in dog and cat fleas in central Oromia, Ethiopia. Am J Trop Med Hyg. 2014;90:457–62. DOIPubMedGoogle Scholar
- Mediannikov O, Abdissa A, Diatta G, Trape JF, Raoult D. Rickettsia felis in fleas, southern Ethiopia, 2010. Emerg Infect Dis. 2012;18:1385–6. DOIPubMedGoogle Scholar
- Keita AK, Socolovschi C, Ahuka-Mundeke S, Ratmanov P, Butel C, Ayouba A, Molecular evidence for the presence of Rickettsia felis in the feces of wild-living African apes. PLoS ONE. 2013;8:e54679. DOIPubMedGoogle Scholar
- Mediannikov O, Davoust B, Socolovschi C, Tshilolo L, Raoult D, Parola P. Spotted fever group rickettsiae in ticks and fleas from the Democratic Republic of the Congo. Ticks Tick Borne Dis. 2012;3:371–3.
- Sackal C, Laudisoit A, Kosoy M, Massung R, Eremeeva ME, Karpathy SE, Bartonella spp. and Rickettsia felis in fleas, Democratic Republic of Congo. Emerg Infect Dis. 2008;14:1972–4. DOIPubMedGoogle Scholar
- Kelly PJ, Mason PR, Matthewman LA, Raoult D. Seroepidemiology of spotted fever group rickettsial infections in humans in Zimbabwe. J Trop Med Hyg. 1991;94:304–9 .PubMedGoogle Scholar
- Parola P. Rickettsia felis: from a rare disease in the USA to a common cause of fever in sub-Saharan Africa. Clin Microbiol Infect. 2011;17:996–1000. DOIPubMedGoogle Scholar
- Roucher C, Mediannikov O, Diatta G, Trape JF, Raoult D. A new Rickettsia species found in fleas collected from human dwellings and from domestic cats and dogs in Senegal. Vector Borne Zoonotic Dis. 2012;12:360–5. DOIPubMedGoogle Scholar
- D’Acremont V, Kilowoko M, Kyungu E, Philipina S, Sangu W, Kahama-Maro J, Beyond malaria—causes of fever in outpatient Tanzanian children. N Engl J Med. 2014;370:809–17. DOIPubMedGoogle Scholar
- Golassa L, Enweji N, Erko B, Aseffa A, Swedberg G. Detection of a substantial number of sub-microscopic Plasmodium falciparum infections by polymerase chain reaction: a potential threat to malaria control and diagnosis in Ethiopia. Malar J. 2013;12:352. DOIPubMedGoogle Scholar
- Males S, Gaye O, Garcia A. Long-term asymptomatic carriage of Plasmodium falciparum protects from malaria attacks: a prospective study among Senegalese children. Clin Infect Dis. 2008;46:516–22. DOIPubMedGoogle Scholar
- Gautret P, Charrel R, Benkouiten S, Belhouchat K, Nougairede A, Drali T, Lack of MERS coronavirus but prevalence of influenza virus in French pilgrims after 2013 Hajj. Emerg Infect Dis. 2014;20:728–30. DOIPubMedGoogle Scholar
- Lundgren IS, Heltshe SL, Smith AL, Chibwana J, Fried MW, Duffy PE. Bacteremia and malaria in Tanzanian children hospitalized for acute febrile illness. J Trop Pediatr. 2015;61:81–5. DOIPubMedGoogle Scholar
- Mediannikov O, Fenollar F, Bassene H, Tall A, Sokhna C, Trape JF, Description of “yaaf,” the vesicular fever caused by acute Rickettsia felis infection in Senegal. J Infect. 2013;66:536–40. DOIPubMedGoogle Scholar
- Edouard S, Bhengsri S, Dowell SF, Watt G, Parola P, Raoult D. Two human cases of Rickettsia felis infection, Thailand. Emerg Infect Dis. 2014;20:1780–1.PubMedGoogle Scholar
- Mediannikov O, Socolovschi C, Million M, Sokhna C, Bassene H, Diatta G, Molecular identification of pathogenic bacteria in eschars from acute febrile patients, Senegal. Am J Trop Med Hyg. 2014;91:1015–9. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 21, Number 10—October 2015
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Didier Raoult, Aix Marseille Université, URMITE, UM63, CNRS 7278, IRD 198, INSERM 1095, Marseille, France
Top