Volume 26, Number 9—September 2020
CME ACTIVITY - Synopsis
Q Fever Osteoarticular Infection in Children
Halima Dabaja-Younis , Michal Meir, Anat Ilivizki, Daniela Militianu, Mark Eidelman, Imad Kassis1, and Yael Shachor-Meyouhas1
, Michal Meir, Anat Ilivizki, Daniela Militianu, Mark Eidelman, Imad Kassis1, and Yael Shachor-Meyouhas1
Figure 3
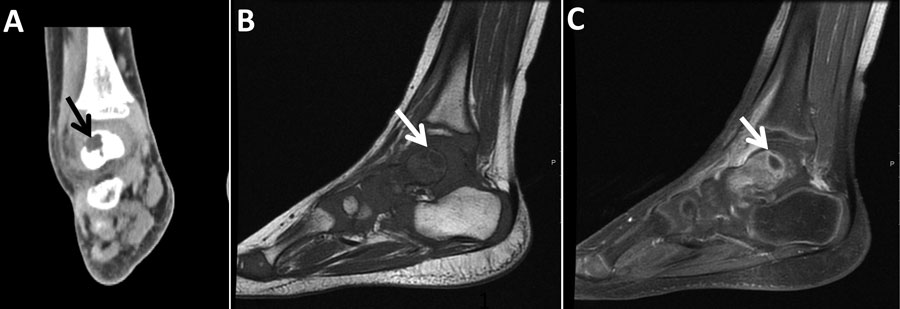
Figure 3. Imaging of the left ankle for a 3-year-old boy (case 3) with Q fever osteoarticular infection, Israel. A) Computed tomography imaging, coronal view, shows a lytic lesion in the talus (black arrow). B, C) Magnetic resonance imaging sagittal T1 (B) and sagittal T1 fat saturation + contrast (C) demonstrate a lesion in the posterior aspect of the talus (white arrows), determined to be an intramedullary abscess (Brodie’s abscess) surrounded by edema.
1These authors contributed equally to the study and article.
Page created: July 02, 2020
Page updated: August 18, 2020
Page reviewed: August 18, 2020
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.