Volume 27, Number 3—March 2021
Research Letter
Severe Pulmonary Disease Caused by Mycolicibacter kumamotonensis
Katerina Manika , Fanourios Kontos, Apostolos Papavasileiou, Dimitrios Papaventsis, Maria Sionidou, and Ioannis Kioumis
, Fanourios Kontos, Apostolos Papavasileiou, Dimitrios Papaventsis, Maria Sionidou, and Ioannis Kioumis
Figure
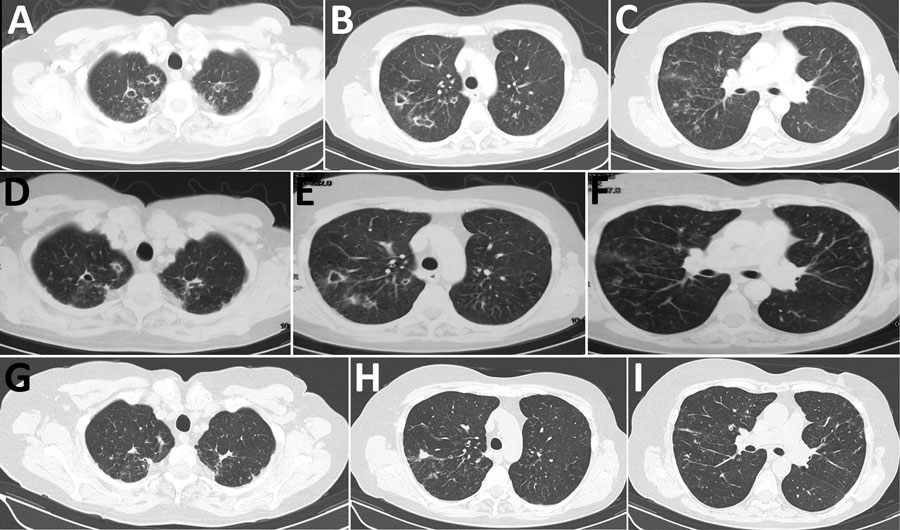
Figure. Chest computed tomography scan 1 month after antituberculosis treatment initiation (A–C), at the time of Mycolicibacter kumamotonensis identification (D–F), and 1 year after treatment initiation for M. kumamotonensis (G–I). Resolution of cavities and scar formation (A to D to G), resolution of pulmonary infiltrations (B to E to H), and hardening of the nodular appearances (C to F to I) are shown.
Page created: November 19, 2020
Page updated: February 22, 2021
Page reviewed: February 22, 2021
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.