Volume 27, Number 4—April 2021
Dispatch
Increased SARS-CoV-2 Testing Capacity with Pooled Saliva Samples
Figure 2
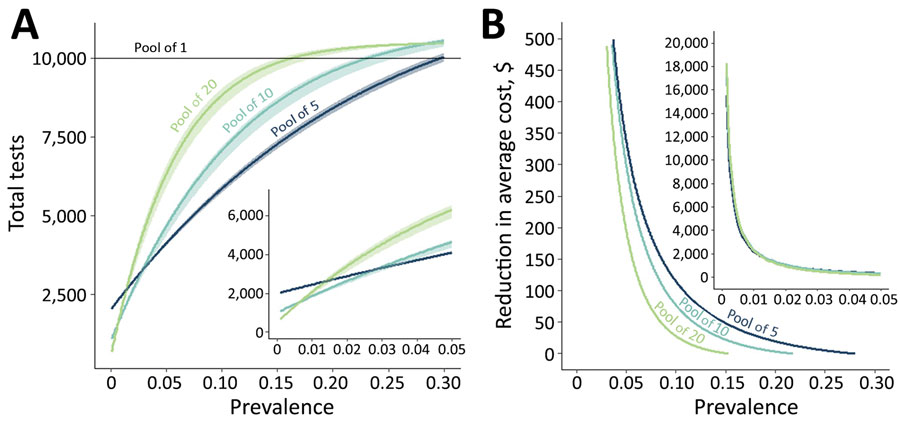
Figure 2. The resource-saving benefit of sample pooling for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing, based on size of the pool and expected prevalence of SARS-CoV-2 within the population. A) We modeled the number of tests required to test 10,000 persons (results qualitatively scale with population) when pools contain 5, 10, or 20 samples (and individually retesting samples within positive pools) compared with testing samples individually (pool = 1 sample). As prevalence increases, so does the number of pools positive for SARS-CoV-2, thereby increasing the required number of confirmatory tests of individual samples. Therefore, over a prevalence of 2.6%, pooled samples of 5 result in fewer overall tests required than do larger pool sizes. B) At lower prevalence rates, such as when outbreaks have been controlled but ongoing screening is required, pools of 10 or 20 samples yield substantial cost savings for the same expected level of positive detections, after accounting for sensitivity differences. Values are shown in US$. Insets show the region with <5% prevalence.
1These senior authors contributed equally to this article.
2Team members team are listed at the end of this article.