Volume 29, Number 9—September 2023
Dispatch
Pharyngeal Co-Infections with Monkeypox Virus and Group A Streptococcus, United States, 2022
Robyn M. Kaiser1 , Shama Cash-Goldwasser1, Nicholas Lehnertz, Jayne Griffith, Alison Ruprecht, John Stanton, Amanda Feldpausch, Jessica Pavlick, Charles A. Bruen, David Perez-Molinar, S. Rebecca Peglow, Omobosola O. Akinsete, Sapna Bamrah Morris, Elliot Raizes, Christopher Gregory, and Ruth Lynfield
, Shama Cash-Goldwasser1, Nicholas Lehnertz, Jayne Griffith, Alison Ruprecht, John Stanton, Amanda Feldpausch, Jessica Pavlick, Charles A. Bruen, David Perez-Molinar, S. Rebecca Peglow, Omobosola O. Akinsete, Sapna Bamrah Morris, Elliot Raizes, Christopher Gregory, and Ruth Lynfield
Figure 2
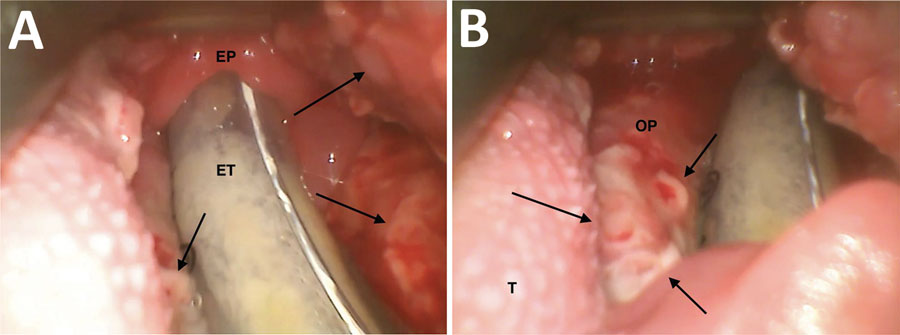
Figure 2. Video laryngoscopy images of patient larynx and pharynx in study of pharyngeal co-infections with monkeypox virus and group A Streptococcus, United States, 2022. A) View of oropharynx, hypopharynx, and laryngeal inlet of patient A (39-year-old man). Arrows indicate mpox lesions. B) Detailed view of mpox lesions. Arrows indicate several lesions. EP, epiglottis; ET, endotracheal tube; OP, oropharynx (lateral wall); T, tongue.
1These first authors contributed equally to this article.
Page created: June 14, 2023
Page updated: August 20, 2023
Page reviewed: August 20, 2023
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.