Volume 3, Number 1—March 1997
Dispatch
The Epidemiology of Creutzfeldt-Jakob Disease in Canada: A Review of Mortality Data
Cite This Article
Citation for Media
Abstract
Creutzfeldt-Jakob disease (CJD), and particularly its transmissibility through blood and blood products, has become a focus of concern in Canada. The recent identification of new variant CJD led to a review of the Canadian mortality database to identify any clustering of CJD by age, sex, or geographic location.
The study by Holman and colleagues (1), which uses mortality data and active surveillance methods, has provided further information on the epidemiology of Creutzfeldt-Jacob disease (CJD). The study concluded that the incidence of the disease in the United States has remained stable and is similar to crude incidence worldwide at about one case per million annually. In addition, the study found no evidence that new variant CJD is present in the U.S. population. These findings are of interest because the epidemiology of CJD in Canada is not well described, and concerns have been raised there about the transmissibility of CJD through transfusion of blood and blood products or through tissue and organ transplants. In addition, many Canadians travel to and from the United Kingdom, where new variant CJD was first identified and linked to the bovine spongiform encephalopathy epidemic (2).
We report here our findings on the epidemiology of CJD in Canada, which are derived from published mortality data (underlying cause of death by standard 5-year age group and sex, for all Canadian residents). The Statistics Canada mortality reports for the years 1979 to 1993 were reviewed for CJD deaths by sex and age group for each province and territory. Reports before 1979 were not used because CJD (ICD-9 code 46.1) was not listed as a cause of death before this time.
Figure 1

Figure 1. Age and sex distribution for Creutzfeldt-Jakob disease in Canada, 1979-1993.
Overall, 334 deaths attributed to CJD were recorded in Canada in the 15-year period from 1979 to 1993, ranging from 14 to 34 deaths per year, with a 1.1:1 male-to-female ratio (Figure 1). Eighty-five percent of the deaths were among persons at least 60 years of age and 50% among the 60- to 69-year-old age group, which corresponds to the peak age of onset of sporadic-type CJD (3-5). Eleven deaths (3%) were reported among persons 30 to 44 years of age. Of these, one death was reported in the 30- to 34-year-old age group, four in the 35- to 39-year-old group, and the remaining six in the 40- to 44-year old age group. No more than one CJD-attributed death was reported per year in the 30- to 44-year-old age groups, with the exception of two deaths reported in 1993. No CJD deaths have been reported among persons under 30 years of age.
Figure 2
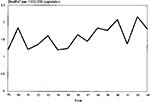
Figure 2. Age-adjusted mortality rate for Creutzfeldt-Jakob disease in Canada, 1979-1993.
Figure 2 shows the mortality rate for CJD in Canada, standardized to the 1979 population. The age-adjusted mortality rate increases from a low of 1.1 deaths per million population in 1979 to a high of 2.1 per million in 1992, dropping to 1.8 per million in 1993. The increase is most marked from 1986 onward. This may be related to increased case recognition following publication of the discovery that CJD was linked to human growth hormone of pituitary origin. A real increase in incidence may also be present, but this graph must be interpreted with caution as the absolute numbers are small and the validity of CJD on death certificates has not been determined in Canada.
Familial-type CJD has been documented in Canada (6,7). As in other countries, most cases of CJD in Canada are of the sporadic type (3-5). One case of iatrogenic CJD was reported in Canada, in a dura mater recipient (8). A review of the Canadian growth hormone recipient database, containing information on the 800 patients who received human growth hormone shows no cases of CJD (Dr. Heather Dean, pers. comm., 1996). Human growth hormone was used in Canada from 1965 until April 1985 (9).
There is one report of a possible cluster of CJD cases in Canada; between April 1989 and October 1990, six cases were reported in the province of Ontario, from a population of 9.5 million (1986 census figure). Two of the patients had come from areas of Czechoslovakia with a high incidence of familial-type disease, but no other risk factors were associated with these cases (7).
In conclusion, the epidemiology of CJD in Canada is not well defined, as current data sources are limited to aggregated mortality data and the annual total case numbers are small. However, several projects have been initiated to provide further information on the transmission of the disease, including an examination of death certificates to identify space/time clustering, active surveillance for CJD and new variant CJD, and a case control study of CJD and blood transfusion.
References
- Holman C, Khan AS, Belay ED, Schonberger LB. Creutzfeldt-Jakob disease in the United States 1979-1994: using national mortality data to assess the possible occurrence of variant cases. Emerg Infect Dis. 1996;2:333–7. DOIPubMedGoogle Scholar
- Will RG, Ironside JW, Zeidler M, Cousens SN, Estibeiro K, Alperovitch A, A new variant of CJD in the UK. Lancet. 1996;347:921–5. DOIPubMedGoogle Scholar
- Brown P, Gajdusek DC. The human spongiform encephalopathies: Kuru, Creutzfeldt-Jakob disease, and the Gerstmann-Straussler-Scheinker syndrome. Curr Top Microbiol Immunol. 1991;172:1–20.
- Brown P, Calatha F, Castaigne P, Gajdusek DC. Creutzfeldt Jacob disease: clinical analysis of a consecutive series of 230 neuropathologically verified cases. Ann Neurol. 1986;20:597–602. DOIPubMedGoogle Scholar
- Will RG. Epidemiology of Creutzfeldt-Jakob disease. Br Med Bull. 1993;49:960–70.PubMedGoogle Scholar
- Goldfarb LG, Brown P, Mitrova E, Cervenakova L, Goldin L, Korczyn AD. Creutzfeldt-Jakob disease associated with the PRNP codon 200LYS mutation: an analysis of 45 families. Eur J Epidemiol. 1991;7:477–86. DOIPubMedGoogle Scholar
- Nosal R, Kapoor A, Shanin R. Cluster of cases of Creutzfeldt-Jakob disease - Ontario. Can Dis Wkly Rep. 1991;17:12.PubMedGoogle Scholar
- Brown P. Environmental causes of human spongiform encephalopathy. In: Baker H, Ridley RM, editors. Methods in Molecular Medicine—Prion Diseases. Totowa (NJ): Humana 1995;139-54.
- Dean HJ, Friesen HG. Growth hormone therapy in Canada: end of one era and beginning of another. Can Med Assoc J. 1986;135:297–301.
Figures
Cite This ArticleTable of Contents – Volume 3, Number 1—March 1997
| EID Search Options |
|---|
|
|
|
|
|
|