Volume 31, Number 2—February 2025
Dispatch
Outbreak of Serotype 1 Invasive Pneumococcal Disease, Kibera Urban Informal Settlement, Nairobi, Kenya, 2023
Cite This Article
Citation for Media
Abstract
Use of 10-valent pneumococcal conjugate vaccine in Kenya has led to substantial reductions in vaccine-type pneumococcal carriage and invasive pneumococcal disease. However, analysis of recent surveillance data indicates an outbreak of vaccine-type serotype 1 in 2023 in Kibera, Kenya. Continued monitoring of invasive pneumococcal disease in Kenya is warranted.
Streptococcus pneumoniae (pneumococcus) is a leading cause of pneumonia, sepsis, and meningitis and is most prevalent in resource-poor settings (1). Pneumococcal serotype 1 (ST1) is an important cause of disease, particularly in sub-Saharan Africa; it is highly invasive and infrequently detected in carriage (2). Pneumococcal conjugate vaccines (PCVs) protect against vaccine-type disease and carriage among vaccinated persons (direct effects), leading to decreased transmission of vaccine serotypes and reduced disease among unvaccinated persons (indirect effects) (3). All currently available PCVs protect against ST1.
In 2011, Kenya introduced 10-valent PCV (Synflorix; GlaxoSmithKline, https://www.gsk.com) (PCV10-GSK), which is administered in 3 doses, at 6, 10, and 14 weeks of age. Vaccine-type invasive pneumococcal disease (IPD) subsequently declined by ≈70%–90%, and vaccine-type carriage declined by ≈50%–60% (3). In 2022, Kenya switched to a newer 10-valent PCV (Pneumosil; Serum Institute of India, https://www.seruminstitute.com) (PCV10-SII).
The Population-Based Infectious Disease Surveillance (PBIDS) platform is implemented in defined catchment populations in Kibera, an urban informal settlement in Nairobi County, and Asembo, a rural area in Siaya County (4); the Kibera site includes ≈25,000 persons in an area ≈1 km2. Through household visits, we collected data on demographics, healthcare use, and vaccination. In both sites, PCV coverage among children <5 years of age has been stably >90%. At centrally located surveillance health facilities (an outpatient clinic in Kibera and an outpatient clinic with small inpatient ward in Asembo), PBIDS participants of all ages meeting standardized criteria for acute febrile illness or severe acute respiratory illnesses (SARI) undergo blood culture; SARI case-patients additionally have a nasopharyngeal swab collected for culture to monitor pneumococcal carriage. The PBIDS protocol was approved by the Kenya Medical Research Institute and the US Centers for Disease Control and Prevention. We obtained written informed consent from participants before sample collection.
We used standard culture procedures to identify pneumococcus. We performed serotyping by real-time PCR, Quellung reaction, or both. At the US Centers for Disease Control and Prevention, we conducted antibiotic susceptibility testing (AST) through broth microdilution (5) for ST1 IPD and carriage isolates from 2023 and short-read whole-genome Illumina sequencing (6). We identified single-nucleotide polymorphisms (SNPs) for core genomes by using kSNP3.0 with k-Mer size of 19 (7) and generated pairwise comparisons by using MEGA version 7 (6,8).
We calculated crude incidence rates and 95% CIs by dividing the number of ST1 bacteremia cases by person-years of observation (PYO). We adjusted incidence rates to account for missed blood samples and healthcare seeking (i.e., cases of medically attended acute febrile illness or SARI reported during household visits for which care was sought at a nonsurveillance facility). We calculated 95% CIs for adjusted incidence rate estimates by using Monte Carlo simulations (0.025 and 0.975 quantiles of 10,000 simulations), sampling from Poisson distribution for crude incidence, and binomial distribution for adjustment factors (9).
We expressed overall and serotype-specific pneumococcal carriage among SARI cases as a percentage, excluding those with limited growth of any organisms, which we deemed poor-quality specimens. We examined ST1 IPD and carriage occurring during January 1, 2018–August 20, 2024. For ST1 isolates from 2023 in Kibera, we described sequence types and AST.
Figure 1
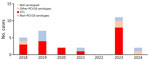
Figure 1. Serotype distribution among invasive pneumococcal disease cases, Kibera Urban Informal Settlement, Nairobi, Kenya, January 1, 2018–August 20, 2024. Other PCV10 serotypes are those common to Synflorix 10-valent PCV (GlaxoSmithKline, ...
Among 4,913 blood samples collected in Kibera, 149 (3.0%) had bacteria isolated, of which 30 (20.1%) were S. pneumoniae. ST1 accounted for 18/30 (60.1%) pneumococcal isolates; 8/18 (44.4%) ST1 isolates were collected in 2023 (Figure 1; Appendix). The crude ST1 IPD incidence rate during 2018–2022 was 8.7 cases/100,000 PYO (95% CI 4.7–16.2 cases/100,000 PYO) versus 35.5 cases/100,000 PYO (95% CI 17.7–71.0 cases/100,000 PYO) in 2023 (Appendix). The adjusted ST1 IPD incidence rate during 2018–2022 was 17.9 cases/100,000 PYO (95% CI 7.3–30.1 cases/100,000 PYO) versus 66.8 cases/100,000 PYO (95% CI 24.8–118.7 cases/100,000 PYO) in 2023 (Appendix). All ST1 IPD case-patients in 2023 were children 2–10 years of age (median 4.5 years of age), and all of them were age-eligible for PCV10-GSK; 5/8 (62.5%) were fully immunized (Table 1). No hospitalizations or fatalities occurred among ST1 case-patients.
Figure 2
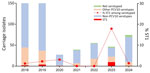
Figure 2. Serotype distribution among invasive pneumococcal disease carriage isolates, Kibera Urban Informal Settlement, Nairobi, Kenya, January 1, 2018–August 20, 2024. Other PCV10 serotypes are those common to Synflorix 10-valent PCV (GlaxoSmithKline, ...
Among serotyped carriage isolates from SARI cases during 2018–2022, 1.5% (7/464) were ST1, and frequency by year ranged from 0 to 3.1% (Table 2; Figure 2). In 2023, 17.9% (10/56) of serotyped carriage isolates from SARI cases in Kibera were ST1.
As of August 20, 2024, we had detected no ST1 IPD cases in 2024, and only 1.3% (1/74) of serotyped carriage isolates were ST1 (Tables 1, 2; Figures 1, 2). We observed no clear increase of ST1 in carriage or IPD in Asembo during the study period (data not shown).
We performed sequencing and AST for 13 ST1 isolates from 2023 (5 IPD and 8 carriage); 9 (69.2%) were sequence type 217, and 4 (30.8%) were sequence type 6056. Genomic analysis demonstrated a 4–15 SNP difference among sequence type 217 isolates and a 6–8 SNP difference among sequence type 6056 isolates, indicating close genomic relatedness. All isolates tested were susceptible to amoxicillin, cefuroxime, and erythromycin; had intermediate susceptibility to penicillin (nonmeningitis oral breakpoint); and were resistant to cotrimoxazole.
Although PCV10-GSK in the Kenya routine infant immunization program has led to substantial reductions in vaccine-type pneumococcal carriage and disease, the surveillance data indicate an outbreak of vaccine-type ST1 in 2023 in Kibera. The IPD case counts from the surveillance area are small, which limits statistical power. However, the ≈4-fold increase in crude and adjusted ST1 IPD incidence rates in 2023 compared with the preceding 5 years, the >10-fold increase in ST1 carriage prevalence (reflecting increased transmission in the community), and the close genetic relatedness of sequenced ST1 isolates from 2023 are consistent with an outbreak. Furthermore, the predominant sequence type detected has been associated with pneumococcal meningitis outbreaks in Malawi (2) and Ghana (10). Pneumococcal disease outbreaks often occur in crowded, closed environments (11); Kibera is densely populated, and the data highlight the risk for IPD outbreaks in urban informal settlements.
ST1 is an important cause of pneumococcal disease outbreaks in sub-Saharan Africa (2). Although PCV implementation has reduced ST1 disease globally (12), several countries, particularly in the meningitis belt, have experienced ST1 IPD outbreaks even in the context of mature PCV programs with high coverage (2). The World Health Organization recommends 3-dose PCV schedules: either 3 primary doses and no booster or 2 primary doses and 1 booster. Booster doses can extend the duration of protection among vaccinated persons. The longer period of direct protection against vaccine serotypes might result in less circulation and more robust indirect protection, particularly against ST1, which frequently affects age groups beyond infancy (13,14). Kenya uses 3 primary doses and no booster schedule; however, if ST1 continues to pose a threat despite high PCV coverage, consideration of switching to 2 primary doses and 1 booster might be merited (14,15). Our data also highlight the importance of optimizing PCV coverage, given that ≈40% of ST1 case-patients in 2023 had not completed PCV vaccination.
Of note, although this outbreak was detected after Kenya switched PCV product from PCV10-GSK to PCV10-SII, all children with ST1 IPD in 2023 were born before 2022 and therefore eligible for PCV10-GSK. Thus, despite the temporal association, the observed increase in ST1 cases in Kibera in 2023 should not be considered a reflection of PCV10-SII performance in Kenya.
All ST1 IPD patients were managed as outpatients, and none died. All ST1 isolates with available AST data were susceptible to first-line treatment for nonsevere pneumonia in Kenya (https://www.researchgate.net/figure/Kenyan-Ministry-of-Health-MoH-guidelines-for-management-of-children-aged-2-59-months_tbl1_264744317).
Preliminary data from 2024 suggest that the ST1 outbreak in Kenya might have resolved. However, continued monitoring of IPD in Kibera and other parts of the country is warranted.
Dr. Komo is an early career researcher at the Kenya Medical Research Institute. Her primary research interest is the epidemiology of infectious diseases with a current focus on pneumococcal diseases.
Acknowledgments
We thank the funders, participants, and field and laboratory teams for their contributions to the study. We also thank Stacy Cobb for her guidance on the analysis.
Funding was provided to Washington State University Global Health Kenya by the US Centers for Disease Control and Prevention (cooperative agreement no. 5U01GH002346) and the Gates Foundation (grant no. INV-009150).
References
- Wahl B, O’Brien KL, Greenbaum A, Majumder A, Liu L, Chu Y, et al. Burden of Streptococcus pneumoniae and Haemophilus influenzae type b disease in children in the era of conjugate vaccines: global, regional, and national estimates for 2000-15. Lancet Glob Health. 2018;6:e744–57. DOIPubMedGoogle Scholar
- Chaguza C, Yang M, Jacques LC, Bentley SD, Kadioglu A. Serotype 1 pneumococcus: epidemiology, genomics, and disease mechanisms. Trends Microbiol. 2022;30:581–92. DOIPubMedGoogle Scholar
- Hammitt LL, Etyang AO, Morpeth SC, Ojal J, Mutuku A, Mturi N, et al. Effect of ten-valent pneumococcal conjugate vaccine on invasive pneumococcal disease and nasopharyngeal carriage in Kenya: a longitudinal surveillance study. Lancet. 2019;393:2146–54. DOIPubMedGoogle Scholar
- Feikin DR, Olack B, Bigogo GM, Audi A, Cosmas L, Aura B, et al. The burden of common infectious disease syndromes at the clinic and household level from population-based surveillance in rural and urban Kenya. PLoS One. 2011;6:
e16085 . DOIPubMedGoogle Scholar - Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing (M100). 33rd edition. Wayne (PA): The Institute; 2023. p. 48–9.
- Metcalf BJ, Chochua S, Gertz RE Jr, Li Z, Walker H, Tran T, et al.; Active Bacterial Core surveillance team. Using whole genome sequencing to identify resistance determinants and predict antimicrobial resistance phenotypes for year 2015 invasive pneumococcal disease isolates recovered in the United States. Clin Microbiol Infect. 2016;22:1002.e1–8. DOIPubMedGoogle Scholar
- Gardner SN, Slezak T, Hall BG. kSNP3.0: SNP detection and phylogenetic analysis of genomes without genome alignment or reference genome. Bioinformatics. 2015;31:2877–8. DOIPubMedGoogle Scholar
- Kumar S, Stecher G, Tamura K. MEGA7: Molecular Evolutionary Genetics Analysis version 7.0 for bigger datasets. Mol Biol Evol. 2016;33:1870–4. DOIPubMedGoogle Scholar
- Hall G, Yohannes K, Raupach J, Becker N, Kirk M. Estimating community incidence of Salmonella, Campylobacter, and Shiga toxin-producing Escherichia coli infections, Australia. Emerg Infect Dis. 2008;14:1601–9. DOIPubMedGoogle Scholar
- Kwambana-Adams BA, Asiedu-Bekoe F, Sarkodie B, Afreh OK, Kuma GK, Owusu-Okyere G, et al. An outbreak of pneumococcal meningitis among older children (≥5 years) and adults after the implementation of an infant vaccination programme with the 13-valent pneumococcal conjugate vaccine in Ghana. BMC Infect Dis. 2016;16:575. DOIPubMedGoogle Scholar
- Zivich PN, Grabenstein JD, Becker-Dreps SI, Weber DJ. Streptococcus pneumoniae outbreaks and implications for transmission and control: a systematic review. Pneumonia. 2018;10:11. DOIPubMedGoogle Scholar
- Bennett JC, Hetrich MK, Garcia Quesada M, Sinkevitch JN, Deloria Knoll M, Feikin DR, et al.; The Pserenade Team. Changes in invasive pneumococcal disease caused by streptococcus pneumoniae serotype 1 following introduction of pcv10 and pcv13: findings from the PSERENADE Project. Microorganisms. 2021;9:696. DOIPubMedGoogle Scholar
- Hausdorff WP, Feikin DR, Klugman KP. Epidemiological differences among pneumococcal serotypes. Lancet Infect Dis. 2005;5:83–93. DOIPubMedGoogle Scholar
- Klugman KP, Madhi SA, Adegbola RA, Cutts F, Greenwood B, Hausdorff WP. Timing of serotype 1 pneumococcal disease suggests the need for evaluation of a booster dose. Vaccine. 2011;29:3372–3. DOIPubMedGoogle Scholar
- Rodgers GL, Whitney CG, Klugman KP. Triumph of pneumococcal conjugate vaccines: overcoming a common foe. J Infect Dis. 2021;224(Suppl 2):S352–9. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: January 16, 2025
Table of Contents – Volume 31, Number 2—February 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Terry Komo, Kenya Medical Research Institute, PO Box 1578-40100, Kisumu, Kenya
Top