Volume 32, Number 2—February 2026
Research Letter
Airport Malaria Cluster in Certified Malaria-Free Country, Libya, 2024
Cite This Article
Citation for Media
Abstract
In November 2024, an autochthonous cluster of 4 Plasmodium falciparum cases (1 fatal) was identified near Benina International Airport, Benghazi, Libya. Epidemiologic and entomologic investigation ruled out local transmission, pointing to airport malaria as the cause and highlighting the vulnerability of malaria-free regions to imported vectors.
Libya, which was certified malaria-free by the World Health Organization in 1973, faces continuous risk for malaria reintroduction from population movements in malaria-endemic regions (1). Although imported cases are occasionally reported, local transmission has not been documented in eastern Libya for >50 years.
On November 28, 2024, the Libya National Centre for Disease Control was notified of a fatal case of Plasmodium falciparum malaria in a 63-year-old resident of Benghazi, Libya, who had no history of travel. Within 48 hours, infection was confirmed in 3 of his children (ages 12, 16, and 23). This familial cluster was located ≈450 meters from Benina International Airport, prompting an investigation to determine the outbreak’s source. This investigation was considered a public health response to an urgent event by the Libya National Center for Disease Control and, as such, was not subject to institutional review board approval. Oral informed consent was obtained from the family members for interviews and testing.
Figure 1
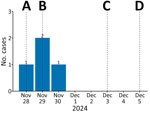
Figure 1. Confirmed malaria cases by symptom onset and public health response timeline in study of airport malaria cluster in certified malaria-free country, Benghazi, Libya, November–December 2024. A) Index case death notified;...
Our investigation defined a case as malaria-like symptoms in a resident near the airport during from mid-November through mid-December 2024 (Figure 1). Active case finding through local healthcare and community outreach identified 20 other suspected patients; all tested negative. All 4 confirmed case-patients, belonging to a single family of 8, were laboratory-confirmed as positive for P. falciparum. None had traveled internationally or received blood transfusions. We formulated 2 primary hypotheses: local transmission from indigenous Anopheles mosquitoes infected by human carrier or airport malaria from an infected Anopheles mosquito imported by aircraft.
Figure 2

Figure 2. Location of airport malaria cluster in certified malaria-free country, Benghazi, Libya, November 2024. The map displays the location of the case cluster (n = 4) and mosquito traps relative to...
To evaluate those hypotheses, we conducted entomological surveillance during November 29–December 2, 2024, deploying National Centre for Disease Control light traps around the family’s residence and within the airport perimeter (Figure 2). We collected 8 mosquitoes, all of which were identified as Culex pipiens. We found no Anopheles mosquitoes, a finding consistent with recent national surveillance data, which documented certain Anopheles species in specific ecologic niches but confirmed their general absence in coastal urban areas such as Benghazi (H. Aqeehal, unpub. data). The absence of competent local vectors enabled us to eliminate local transmission, making airport malaria the most plausible explanation (2).
This investigation concluded that an infected anopheline mosquito was likely imported by aircraft, probably within cargo given the absence of recent passenger flights from malaria-endemic areas, and subsequently infected members of a family living nearby. Although importation of vectors overland through migrant routes is a theoretical possibility (3,4), the acute, geographically tight cluster in a nonmigrant family points strongly toward a point-source introduction at the airport.
This event is a critical reminder that malaria-free status does not eliminate risk, because points of entry are permeable frontiers for vectorborne diseases (5,6). Our findings prompted immediate recommendations to Libya health authorities to strengthen entomologic surveillance at points of entry and rigorously enforce aircraft and cargo disinsection protocols in accordance with the World Health Organization’s International Health Regulations (2005) (7). We also emphasize the need for clinicians near airports to consider malaria in patients with fever, regardless of travel history. The vulnerability of nonendemic regions requires constant vigilance to prevent the reestablishment of malaria.
Dr. Alarbi is a fellow of the Mediterranean and Black Sea Programme in Intervention Epidemiology Training at the National Center for Disease Control, Tripoli, Libya. His primary research interest is the epidemiology of emerging and vectorborne diseases in North Africa.
Acknowledgments
The authors collectively thank the staff at the Benghazi Medical Center and the field and laboratory teams at the National Center for Disease Control for their timely response and unwavering dedication during this investigation. We are also grateful to our colleagues in the European Centre for Disease Prevention and Control (ECDC) Project Review Module for their invaluable feedback, which significantly improved this manuscript. A.A. wishes to extend his personal gratitude to his frontline coordinator, Pawel Stefanoff, for his continuous guidance, and to his supervisor, Zeinab Saleh, for her expert mentorship and steadfast support throughout this project.
ChatGPT-4 (OpenAI, November 2023 version) was used to assist with language editing, formatting, and refining the manuscript for clarity and adherence to journal guidelines.
A.A. is a fellow of the MediPIET program, supported financially by the ECDC. The views and opinions expressed herein do not state or reflect those of ECDC. ECDC is not responsible for the data and information collation and analysis and cannot be held liable for conclusions or opinions drawn.
References
- Gebreel AO, Gilles HM, Prescott JE. Studies on the sero-epidemiology of endemic diseases in Libya, IV. Malaria. Ann Trop Med Parasitol. 1985;79:341–7. DOIPubMedGoogle Scholar
- Kessel J, Rosanas-Urgell A, Dingwerth T, Goetsch U, Haller J, Huits R, et al. Investigation of an airport-associated cluster of falciparum malaria in Frankfurt, Germany, 2022. Euro Surveill. 2024;29:
2300298 . DOIPubMedGoogle Scholar - Tabbabi A, Alkishe AA, Samy AM, Rhim A, Peterson AT. Malaria in North Africa: a review of the status of vectors and parasites. J Entomol Sci. 2020;55:25–37. DOIGoogle Scholar
- Nebbak A, Almeras L, Parola P, Bitam I. Mosquito vectors (Diptera: Culicidae) and mosquito-borne diseases in North Africa. Insects. 2022;13:962. DOIPubMedGoogle Scholar
- Schlagenhauf P, D’Acremont V, Buhler S, Hatz C. Airport malaria and odyssean malaria. In: Keystone A, Kozarsky P, Connor B, Nothdurft H, Mendelson M, Cartwright K, editors. Travel medicine. 4th ed. Philadelphia: Elsevier; 2019. p. 64–7.
- Ibáñez-Justicia A, Smitz N, den Hartog W, van de Vossenberg B, De Wolf K, Deblauwe I, et al. Detection of exotic mosquito species (Diptera: Culicidae) at international airports in Europe. Int J Environ Res Public Health. 2020;17:3450. DOIPubMedGoogle Scholar
- World Health Organization. International Health Regulations (2005). 3rd ed. Geneva: The Organization; 2016.
Figures
Cite This ArticleOriginal Publication Date: February 17, 2026
Table of Contents – Volume 32, Number 2—February 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Ahmed Alarbi, National Center for Disease Control, Zawiat Aldahmani, Bldg 6, Apt 16, Tripoli 1040, Libya
Top