Volume 32, Number 4—April 2026
Dispatch
Outbreak of Dengue Virus Serotype 3, Republic of the Marshall Islands, 2019–2021
Cite This Article
Citation for Media
Abstract
During 2019–2021, the Republic of the Marshall Islands experienced a dengue outbreak involving 1,908 cases. Environmental sanitation helped stop transmission on Ebeye island, but transmission continued for >1 year on Majuro atoll. The Pacific region urgently needs to develop vector control capacity to address future dengue outbreaks.
Dengue, caused by dengue virus (DENV), is a vectorborne disease transmitted by Aedes spp. mosquitoes. DENV has 4 major serotypes (1–4); infection with one serotype protects against future infection with that serotype but leads to antibody-dependent enhancement and potentially more severe disease upon infection with a heterologous serotype (1).
The primary global dengue vector is the Ae. aegypti mosquito, which has a widespread and ever-expanding range (2). In the Western Pacific, Ae. albopictus, Ae. polynesiensis, and Ae. hensili dengue vectors coexist with Ae. aegypti (3). Some Pacific Island countries and territories are dengue-endemic, but many others have periodic outbreaks in which DENV presumably is introduced by travelers returning from endemic areas (4). Introduction via infected mosquitoes brought by plane or boat also is possible and difficult to definitively rule out (4). In the Pacific, most DENV introductions are thought to be from returning residents rather than visiting tourists.
Before 2019, the last major dengue outbreak in the Republic of the Marshall Islands (RMI) was during 2011–2012 and involved DENV-4 (5). The attack rate (AR) during that outbreak was 1.6% among laboratory-confirmed cases, and suspected AR was 3% (5). In that outbreak, 95% of tested samples (50% in children 0–4 years of age, 80% in children 5–9 years of age, >90% in persons >10 years of age) had evidence of secondary infection, showing a history of substantial DENV circulation in RMI (5).
Figure
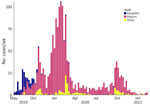
Figure. Number of confirmed cases per atoll in an outbreak of dengue virus serotype 3, Republic of the Marshall Islands, 2019–2021. Bars show weekly case counts. Although the first case was...
On May 15, 2019, a dengue case was identified in a patient on Ebeye island in the Kwajalein atoll of RMI. The case-patient had no travel history outside RMI. Another suspected case occurred on Ebeye on June 4, 2019. Subsequently, case counts rapidly increased and were detected across much of RMI, mainly on Kwajalein and Majuro atolls (Figure). Serotyping showed the outbreak was caused by DENV-3, which had not been recorded in RMI for 30 years, although DENV-3 possibly circulated in RMI during the mid-1990s or early 2000s (6). To investigate effectiveness of vector control strategies, we compared dengue ARs between the island of Ebeye, where systematic, islandwide vector control began soon after case detection, and the Majuro atoll, where human disease and vector surveillance is not routinely conducted.
In response to dengue case detections, the Ministry of Health and Human Services (MOHHS) and the RMI Environmental Protection Authority (RMIEPA) initiated vector control activities across Ebeye on July 16, 2019. Ebeye government officials also began islandwide cleanup campaigns when dengue cases began increasing. RMIEPA used BG-Sentinel Mosquito Traps (Biogents, https://eu.biogents.com) for surveillance of adult mosquitoes and larvae or pupae to check for vectors before applying pesticides, when possible. Ae. aegypti mosquitoes were the only dengue vector found on Ebeye.
On Ebeye, RMIEPA applied indoor and outdoor residual adulticide bifenthrin or deltamethrin spray, and pyriproxyfen or Bacillus thuringiensis larvicide, on the basis of the larval survey, following the manufacturer’s labels. The vector assessment found Ae. aegypti mosquitoes in containers in about half of homes inspected (Table 1); the most productive larval mosquito containers were drums for storing water, mainly used for washing, not drinking.
On August 6, 2019, the RMI government declared a state of emergency for the entire territory. MOHHS provided vector management efforts against Aedes spp. mosquito breeding sites through community engagement campaigns, including informational radio spots, social media posts, press reporting, and advocacy by traditional and ecclesial leaders. MOHHS and RMIEPA provided vector control to households with suspected and confirmed dengue cases.
PCR testing for RMI is only available in Hawaii, USA, as is common for many Pacific islands, so most (82%) confirmatory test results were ELISA of the nonstructural protein 1 antigen, 18% were DENV IgM, and <1% were PCR. Of note, most (59%) confirmed cases were among children 5–17 years of age (Table 2); however, only 44% of patients experiencing dengue-like illness during the outbreak were 5–17 years of age (Table 3).
Ebeye, where earliest dengue activity for this outbreak occurred, comprises ≈23% of the RMI population (7). By October 2019, case counts on Ebeye declined, and most dengue activity occurred on Majuro atoll, where ≈55% of the RMI population resides (7). Other atolls with documented cases were Ailinglaplap, Arno, Aur, Enewetak, Jaluit, Kili, Maloelap, Mili, Namu, Utrik, and Wotje. The overall dengue AR on Ebeye island was 1.3%, compared with the 7.1% AR on Majuro atoll, where vector control was only initiated in response to confirmed case identifications. After a spike in detected DENV transmission during December 2019–March 2020, dengue persisted on Majuro atoll with decreased case activity during March–September 2020 before cases increased in again in late 2020, preceding the eventual end of the outbreak in February 2021 (Figure).
RMIEPA conducted mosquito surveys on Majuro and other atolls, including Ailinglaplap, Arno, Aur, Enewetak, Jaluit, Kili, Kwajalein, Maloelap, Mili, and Wotje atolls, which confirmed Ae. aegypti, Ae. albopictus, and Ae. marshallensis mosquito vectors. Of note, those atolls had dengue ARs similar to Majuro. Although RMIEPA did not conduct mosquito surveys on Namu and Utrik atolls, the agency suspects those atolls likely had >1 of the Aedes spp. mosquito vectors.
The final confirmed case associated with this outbreak was recorded on February 20, 2021, resulting in a total of 1,908 laboratory-confirmed cases, among which 716 case-patients were hospitalized and 2 died. Officially, the dengue outbreak lasted 21 months, overlapping with the beginning of the COVID-19 global pandemic and associated travel restrictions that halted most international and intraisland travel beginning in March 2020. Of note, most dengue cases on Ebeye occurred in the first 2 months of the outbreak, suggesting successful vector control kept the overall AR low at 1.3%, compared with the 7.1% AR on Majuro atoll. Vector control was only initiated on Majuro in response to positive case identification, and DENV transmission persisted on the atoll. Recommendations by the US Centers for Disease Control and Prevention and the Pacific Island Health Officers Association for future dengue prevention and control efforts on the basis of the vector assessment included continued capacity building, environmental sanitation through improved waste management, chemical vector control, and improved domestic water collection and storage.
RMI experienced an extended dengue outbreak during 2019–2021, overlapping with COVID-19 restrictions, suggesting that local transmission was sustained throughout the period unaided by additional case introductions. Initial cases were concentrated on Ebeye island in Kwajalein atoll, where vector control and environmental health activities helped mitigate local mosquito populations and curtail DENV transmission. Transmission persisted in Majuro atoll for an additional 18 months. Of note, Majuro is 4 times more densely populated than Kwajalein atoll (7), likely another contributing factor to the sustained transmission on Majuro compared with Kwajalein during this outbreak. The 2011–2012 dengue outbreak in RMI showed a similar AR between Kwajalein and Majuro (5). Compared with the 2011–2012 outbreak, confirmed dengue cases in the 2019–2021 outbreak had a younger age distribution and a higher concentration of cases in children 5–17 years of age. The relative lack of burden in the adult population suggests possible DENV-3 transmission in RMI in the 1990s, when that population might have experienced infection and therefore acquired immunity.
In summary, distribution of dengue cases across multiple atolls, several with high ARs, highlights the challenges for outbreak control in the Pacific and other regions where human disease and vector surveillance is not conducted regularly and systematically. Vector control and environmental health efforts on Ebeye successfully averted further DENV-3 transmission. Those findings support the need for building vector control capacity in the Pacific, where dengue outbreaks of this scale are likely to continue.
Dr. León conducted this research as an early warning system consultant for the Pacific Island Health Officers’ Association. His primary research interests focus on applying modeling and advanced analytic methods to support dengue outbreak preparedness and response in the Pacific.
Acknowledgments
We thank Dominic Rose for completing the Ebeye larval surveys, Jackson Jacklick for the vector management, and the numerous partners who worked tirelessly during this response effort.
This work was conducted as part of surveillance and outbreak response activities of the Republic of the Marshall Islands Ministry of Health and Human Services (RIM-MOHHS). Per advisement by RMI-MOHHS institutional review board, these activities are not considered human subjects research; thus, institutional review board review and approval were not required.
T.M.L. and L.K.H. were partly funded by a grant to the Pacific Island Health Officers’ Association from the US Department of State (cooperative agreement no. SLMAQM20CA2490). The opinions, findings, and conclusions stated herein are those of the authors and do not necessarily reflect those of the US Department of State.
References
- Paz-Bailey G, Adams LE, Deen J, Anderson KB, Katzelnick LC. Dengue. Lancet. 2024;403:667–82."https://pubmed.ncbi.nlm.nih.gov/38280388" \h DOIPubMedGoogle Scholar
- Kraemer MUG, Reiner RC Jr, Brady OJ, Messina JP, Gilbert M, Pigott DM, et al. Past and future spread of the arbovirus vectors Aedes aegypti and Aedes albopictus. Nat Microbiol. 2019;4:854–63."https://pubmed.ncbi.nlm.nih.gov/30833735" \h DOIPubMedGoogle Scholar
- Russell TL, Burkot TR. A guide to mosquitoes in the Pacific. Cairns (Australia): Pacific Community; 2023.
- Matthews RJ, Kaluthotage I, Russell TL, Knox TB, Horwood PF, Craig AT. Arboviral disease outbreaks in the Pacific Islands countries and areas, 2014 to 2020: a systematic literature and document review. Pathogens. 2022;11:74."file:///\\\\cdc.gov\\project\\CCID_NCPDCID_DEISS_EIDJ\\EID%20Production\\Editorial\\EDITING\\Amy\\4-Apr-2026\\D25-1135%20DENV\\PubMed" DOIPubMedGoogle Scholar
- Sharp TM, Mackay AJ, Santiago GA, Hunsperger E, Nilles EJ, Perez-Padilla J, et al. Characteristics of a dengue outbreak in a remote pacific island chain—Republic of The Marshall Islands, 2011-2012. PLoS One. 2014;9:
e108445 . DOIPubMedGoogle Scholar - Singh N, Kiedrzynski T, Lepers C, Benyon EK. Dengue in the Pacific—an update of the current situation. Pac Health Dialog. 2005;12:111–9. PubMedGoogle Scholar
- Marshall Islands Economic Policy, Planning and Statistics Office. Republic of the Marshall Islands 2021 census report [cited 2025 Feb 18]. https://rmihealth.org/media/attachments/2025/08/08/marshall_islands_2021_census_vol1_table_report.pdf
Figure
Tables
Cite This ArticleOriginal Publication Date: April 09, 2026
Table of Contents – Volume 32, Number 4—April 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Tomás M. León, Pacific Island Health Officers’ Association, 733 Bishop Street, Suite 1820, Honolulu, HI 96813, USA
Top