Volume 32, Number 7—July 2026
Dispatch
Vascularized Iris Mass as Sentinel Manifestation of Syphilis in Patient with HIV Infection, Spain, 2025
Cite This Article
Citation for Media
Abstract
Vascularized iris masses are rare, yet highly suggestive of syphilis. We report a 51-year-old man in Spain with HIV infection who had painful vision loss, rash, and an iris mass. Laboratory testing confirmed syphilis; ocular manifestations resolved with intravenous ceftriaxone and penicillin. Early recognition of syphilis can prevent vision loss and neurologic complications.
Syphilis has experienced an alarming global resurgence over the past 2 decades, evolving into a major public health concern across developed nations (1). Ocular syphilis, known as the great masquerader, can involve any ocular structure and can occur at any stage of the disease; ocular syphilis frequently serves as the sentinel manifestation of an undiagnosed HIV infection (2,3). Although uveitis is the most common manifestation of ocular syphilis, vascularized iris masses, spanning a clinical spectrum from iris roseola and papulosa to iris nodosa and gummata, represent an exceptionally rare and poorly characterized phenotype (4). Fewer than 15 cases have been reported in English-language literature (5–8), and paradoxically, despite the synergy between syphilis and HIV infection, iris lesions are even more infrequent in persons with advanced immunosuppression (9).
The formation of structured nodules or gummata typically represents an inadequate or failed delayed-type hypersensitivity (DTH) reaction (8). Differential diagnosis is challenging because the lesions can mimic other inflammatory, neoplastic, or opportunistic fungal processes in patients with HIV. Multimodal ultrasound biomicroscopy (UBM) imaging and anterior segment optical coherence tomography (AS-OCT) can aid in lesion characterization, defining depth, internal composition, vascularity, and stromal involvement (5,8). We report a case of iris papulosa as a sentinel sign of syphilis in a patient in Spain with HIV infection.
Figure 1
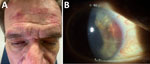
Figure 1. Clinical findings of a vascularized iris mass as sentinel manifestation of syphilis in patient with HIV infection, Spain, 2025. A) Maculopapular facial rash consistent with secondary syphilis. B) Slit-lamp photograph...
Figure 2
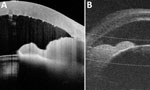
Figure 2. Imaging for a vascularized iris mass as sentinel manifestation of syphilis in patient with HIV infection, Spain, 2025. A) Ultrasound biomicroscopy revealing a well-defined hyperechoic iris mass with ciliary body...
In 2025, a 51-year-old man with a history of HIV, depression, and substance abuse (amphetamines and cocaine) sought care for 3 days of right-eye pain and vision loss. Facial maculopapular rash suggested secondary syphilis (Figure 1, panel A). Best-corrected visual acuity was hand motion in the right eye and 20/20 in the left eye. Intraocular pressures were 8 mm Hg in the right eye and 10 mm Hg in the left eye. Slit-lamp examination of the right eye revealed marked conjunctival hyperemia, a vascularized nonpigmented iris base mass, corneal edema, mutton-fat keratic precipitates, posterior synechiae, and 3+ anterior chamber cells and flare (Figure 1, panel B). Ocular ultrasonography ruled out vitreous inflammation and retinal detachment. UBM revealed a well-defined, homogeneous hyperechoic iris stromal mass with ciliary body involvement and iris pigment epithelium disruption (Figure 2, panel A). AS-OCT demonstrated a homogeneous lesion with irregular hyperreflective anterior surface, internal hyperreflectivity, posterior shadowing, iris pigment epithelium disruption, keratic precipitates, and anterior chamber cells (Figure 2, panel B).
Ocular syphilis was confirmed by rapid plasma regain (titer 1:256) and positive Treponema pallidum microparticle enzyme immunoassay. Lumbar puncture was performed, and cerebrospinal fluid tested T. pallidum–negative. HIV viral load was 25 copies/mL; CD4+ cell count was 13% (300 cells/μL). HIV history was unavailable because of poor follow-up; the patient reported intermittent, poorly adherent antiretroviral therapy but was taking it during uveitis diagnosis, which explains viral suppression despite persistent immunosuppression. No viral loads or CD4 counts were available from the previous year. Serologic tests for tuberculosis, sarcoidosis, hepatitis, and toxoplasmosis were negative.
We administered intravenous ceftriaxone (2 g/d for 5 d) as an initial bridging therapy at home while we arranged logistics for in-home intravenous penicillin G (18 million units/d for 10 d) (10). Adjunctive therapy included 1% topical prednisolone acetate (4×/d), 1% cycloplegic agent (atropine; 2×/day, and systemic prednisone initiated at 30 mg/day and tapered over 2 weeks. At 1 month, best-corrected visual acuity recovered to 20/20, and repeat UBM and AS-OCT confirmed complete lesion resolution in the right eye.
Ocular syphilis most commonly occurs during the secondary stage of T. pallidum infection (6). Among its diverse phenotypes, vascularized iris masses, including iris roseola, papulosa, nodosa, and gummata, are considered exceptional but highly suggestive of treponemal disease (5,6). Such lesions are thought to result from T. pallidum capillary engorgement or focal inflammatory infiltration, representing a spectrum of progressively intensifying inflammatory responses (6). Iris roseola, the earliest manifestation in secondary syphilis, consists of dilated capillaries or vascular tufts and can evolve into iris papulosa, single or multiple nodules, and subsequent iris nodosa, reflecting increasing granulomatous stromal infiltration (5,7,11). In contrast, iris gummata typically occur in later stages, presenting as poorly vascularized nodules with central degeneration that represent chronic granulomatous inflammation associated with impaired cellular immune control (5,6,8).
In a comprehensive review of reports published in English, we identified only ≈13 cases of vascularized iris masses documented since 1915 (5–9) (Appendix Table). One case of a large syphilitic iris granuloma in a patient with HIV infection has been highlighted in recent reviews, whereas most published cases occurred in patients without HIV or with unreported HIV status (9) (Appendix Table).
The co-occurrence of syphilitic iris nodules and HIV infection appears paradoxically rare. Despite the epidemiologic synergy between HIV and syphilis, iris granulomas are reported less often among persons with HIV infection than in immunocompetent hosts (12). Gummata represent chronic granulomatous lesions arising from a failure of effective DTH reaction to T. pallidum, reflecting impaired cellular immune control (8). In HIV infection with CD4+ depletion, the immune system might lack the capacity for such granulomatous responses (13). Consequently, syphilis in patients with HIV more frequently manifests as severe, diffuse inflammation or posterior segment involvement, rather than discrete iris nodules (12,13). The pronounced granulomatous iris mass in this patient, despite CD4+ of 300 cells/μL, suggests residual capacity for granuloma formation despite DTH impairment, possibly due to partial immune reconstitution or localized immune responses.
In patients with HIV, a solitary vascularized iris mass substantially broadens the differential diagnosis. Syphilitic nodules must be distinguished from neoplastic entities, other infections, or inflammatory causes (8,14). Among neoplastic causes, iris nevus typically presents as a flat or minimally elevated, well-circumscribed pigmented lesion with slow growth and is usually asymptomatic, whereas iris melanoma tends to be more elevated and might exhibit intrinsic vascularity, corectopia, uveal ectropion, and progressive enlargement. Iris metastases are typically amelanotic and often identified in patients with a known primary tumor (15). Intraocular lymphoma, although less common, can appear as diffuse iris infiltration, often accompanied by chronic inflammation. Infectious causes of iris granulomas include ocular tuberculosis in the setting of chronic granulomatous uveitis, often with systemic involvement (5,15).
Anterior segment imaging can support diagnostic evaluation by helping define lesion depth and internal characteristics, thereby contributing to the differential diagnosis among inflammatory, neoplastic, and alternative infectious causes. However, the diagnosis of ocular syphilis remains primarily clinical and serologic, and imaging findings can further aid in lesion characterization and monitoring treatment response (5,6).
Vascularized iris masses represent an exceptionally rare manifestation of ocular syphilis; only ≈13 cases have been reported in the literature, and just 1 previous case was described in a patient with HIV co-infection. Our case demonstrates that, even in HIV infection, syphilis manifestations can present as a localized anterior segment mass rather than diffuse ocular inflammation. Internists and infectious disease physicians should be aware that an unexplained iris mass, particularly in patients at risk for sexually transmitted infections, could represent syphilis. Prompt serologic testing and appropriate parenteral therapy are essential to preventing irreversible visual and neurologic complications.
Dr. Caminal-Caramés is an ophthalmologist at Hospital Sant Pau, Barcelona, Spain. Her research interests include retina, uveitis and ocular inflammation diseases, retinal dystrophies, and pediatric retina disorders.
Acknowledgment
The authors certify that they obtained all appropriate patient consent forms. In the form, the patient gave consent for his images and other clinical information to be reported in the journal, signing a written informed consent. All procedures were performed in accordance with the principles expressed in the Declaration of Helsinki.
References
- Zhou LR, Kirupaharan N, Berkenstock MK. Incidence and prevalence of syphilitic uveitis and associated ocular complications in the TriNetX database. Am J Ophthalmol. 2025;277:387–94. DOIPubMedGoogle Scholar
- Lee SY, Cheng V, Rodger D, Rao N. Clinical and laboratory characteristics of ocular syphilis: a new face in the era of HIV co-infection. J Ophthalmic Inflamm Infect. 2015;5:56. DOIPubMedGoogle Scholar
- Amaratunge BC, Camuglia JE, Hall AJ. Syphilitic uveitis: a review of clinical manifestations and treatment outcomes of syphilitic uveitis in human immunodeficiency virus-positive and negative patients. Clin Exp Ophthalmol. 2010;38:68–74. DOIPubMedGoogle Scholar
- Schulz DC, Orr SMA, Johnstone R, Devlin MK, Sheidow TG, Bursztyn LLCD. The many faces of ocular syphilis: case-based update on recognition, diagnosis, and treatment. Can J Ophthalmol. 2021;56:283–93. DOIPubMedGoogle Scholar
- Rosenberg CR, Pasadhika S. A vascularized iris mass in ocular syphilis: a case report and review of literature. Ocul Immunol Inflamm. 2024;32:1648–54. DOIPubMedGoogle Scholar
- Chen JL, Tessema R, Emami-Naeini P, Lim MC. A vascular syphilitic iris lesion. Am J Ophthalmol Case Rep. 2023;31:
101858 . DOIPubMedGoogle Scholar - de Jong Y, Haverkort ME, van Sorge AJ, Jansen C, Luyten GP, Joosse M. A translucent vascularised iris granuloma in a patient with secondary syphilis. Lancet Infect Dis. 2017;17:255–6. DOIPubMedGoogle Scholar
- Michaelov E, Iqbal MM, Hooper PL. Uveal mass, uveitis, and diffuse rash in a woman in her 50s. JAMA Ophthalmol. 2018;136:704–5. DOIPubMedGoogle Scholar
- Yang P, Zhang NI, Li F, Chen Y, Kijlstra A. Ocular manifestations of syphilitic uveitis in Chinese patients. Retina. 2012;32:1906–14. DOIPubMedGoogle Scholar
- Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70:1–187. DOIPubMedGoogle Scholar
- Bociąga-Kożuch M, Raczyńska A, Trela D, Garlicki A, Berus T. Diagnostic riddle—case report of ocular syphilis. J Ophthalmic Inflamm Infect. 2025;15:33. DOIPubMedGoogle Scholar
- Balba GP, Kumar PN, James AN, Malani A, Palestine AG, Welch JN, et al. Ocular syphilis in HIV-positive patients receiving highly active antiretroviral therapy. Am J Med. 2006;119:448.e21–5. DOIPubMedGoogle Scholar
- Carlson JA, Dabiri G, Cribier B, Sell S. The immunopathobiology of syphilis: the manifestations and course of syphilis are determined by the level of delayed-type hypersensitivity. Am J Dermatopathol. 2011;33:433–60. DOIPubMedGoogle Scholar
- Tasnim S, Dave D, Tawfeeq Y, Naguib T, Rasheed W. A case of ocular neurosyphilis in a patient with HIV. Southwest Respir Crit Care Chron. 2021;9:44–6. DOIGoogle Scholar
- Moshirfar M, Rageh A, Ronquillo Y. Benign and malignant iris tumors. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
Figures
Cite This ArticleOriginal Publication Date: June 17, 2026
Table of Contents – Volume 32, Number 7—July 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Marta Caminal-Caramés, Ophthalmology Department, Hospital Sant Pau, C/Sant Quintí 89, Barcelona 08025, Spain
Top