Volume 4, Number 2—June 1998
Dispatch
Using Nurse Hot Line Calls for Disease Surveillance
Cite This Article
Citation for Media
Abstract
Nurse hot line calls are a potential source of public health surveillance data and may help identify epidemics of emerging infectious diseases. In this study, nurse hot line data from Milwaukee, Wisconsin, showed more than a 17-fold increase in calls for diarrhea during the 1993 Milwaukee cryptosporidiosis outbreak. Moreover, consistent patterns of seasonal variation in diarrhea- and vomiting-related calls were detected from the Baltimore, Maryland, and Albuquerque, New Mexico, hot lines. Analysis of nurse hot line calls may provide an inexpensive and timely method for improving disease surveillance.
Most disease outbreaks are identified by an alert health care provider or citizen (1-3); some are identified by analyses of laboratory-confirmed reportable diseases (4,5) in these outbreaks, because of delays in specimen collection and analysis, laboratory confirmation is often received by public health agencies days to weeks after the onset of illness, and consequently, outbreak investigations are delayed. Some outbreaks may not be detected at all because of limitations of the disease surveillance system (6). Several new surveillance methods for more timely detection of outbreaks have been proposed (6,7). Among these is the analysis of calls to nurse hot lines, also known as nurse call lines.
During the past 5 years, computerized hot line systems for sorting patient calls have been developed and marketed. Patient calls concerning illness or injury are received by trained nurses, who categorize symptoms and provide advice on the basis of approved protocols. The computerized hot line systems integrate structured interview, record keeping, and treatment protocol. These systems have been expanding one nurse hot line vendor alone has installed more than 240 systems throughout the United States and Canada. These systems have been highly successful not only because they provide patient services, but also because they save physicians' time (8-10).
During the structured interview, nurses follow symptom-based guidelines developed by the software vendors and modified and approved by local physicians. As part of the interview process, information about the illness and the patient is computerized and can usually be retrieved with minimal cost. For example, two hot line systems in Albuquerque, New Mexico, receive more than 50,000 calls each per year; the systems' software can provide summary reports of calls. A major advantage of nurse hot line systems for disease surveillance is, therefore, their ability to provide timely information from a large number of callers. Disadvantages are that hot lines provide symptom-based rather than pathogen-based reports and that persons who call several times can be counted as separate callers. For hot lines connected with health maintenance organizations, the data may be expressed in terms of the population, whereas call systems that serve an unknown number of clients cannot.
Our study, which provides preliminary data on the potential value of nurse hot line data for disease surveillance, had two specific goals: to evaluate whether nurse hot line calls for diarrhea-related illness during the 1993 Milwaukee cryptosporidiosis outbreak increased and could have identified the outbreak earlier than other methods and to evaluate whether nurse hot line calls for diarrheal diseases reflected an expected seasonal variation.
We telephoned directors of three nurse hot lines: Covenant Healthcare System (CHS), Milwaukee, Wisconsin; Lovelace Health Hot Line (LHH), Albuquerque, New Mexico; and Helix Telehealth Center (THC), Baltimore, Maryland; they agreed to provide hot line call data at no cost. CHS and THC used the Ask-A-Nurse system, which defined diarrhea as a sudden increase in number and volume of bowel movements causing rapid evacuation of water and electrolytes. When the caller described multiple symptoms, detailed guidelines were used to choose the major symptom, and the call was documented in only one category. LHH used the Sharp Focus System and defined diarrhea as five or more watery stools every 6 hours. Records of daily CHS adult and pediatric (age < 13 years) diarrhea-related calls for two Milwaukee hospitals were examined for the period March 4 to May 10, 1993, to determine whether the number of calls increased during the cryptosporidiosis outbreak (11). Hot line calls to LHH and THC from July 1994 to July 1996 for pediatric (ages < 13 years) diarrhea and adult (ages > 18 years) vomiting were plotted for each month. Temporal patterns of calls for respiratory conditions and skin rashes were also examined.
Figure 1
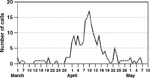
Figure 1. Calls to Covenant Healthcare System hot line, Milwaukee, Wisconsin, March 1–May 10, 1993.
From March 1 to April 1, 1993, and from April 25 to May 10, 1993, the CHS hot line in Milwaukee received an average of 0.66 adult diarrhea calls per day. An increase in diarrhea calls more than four standard deviations higher than the background rate (p < 0.001) was noted on April 2 (Figure 1), 4 days before a television news story about dramatic increases in cases of diarrhea (7). The number of calls remained high through April 16, with a peak in adult calls on April 10, 3 days after the Milwaukee Health Department reported the outbreak. Adult diarrhea calls peaked at more than 17 times the average number of calls received per day before and after the outbreak and returned to this number on April 25. Pediatric diarrhea-related calls increased from 18 in March to 38 in April and declined to 17 in May and 11 to 14 per month from June through August (not shown).
Analysis of the calls by zip code indicated that most callers lived near the two hospitals (located in the north and northwest parts of the city), which were least affected by the outbreak. These data may not represent illness rates in different parts of the city.
Figure 2
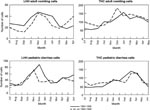
Figure 2. Seasonal variation of calls to Lovelace Health Hot Line (LHH) and Helix Telehealth (THC), 19941996.
To determine whether hot line calls reflect seasonal disease patterns, adult vomiting- and pediatric diarrhea-related calls to the THC and LHH hot lines were plotted for 24 consecutive months (Figure 2). Each condition showed a strong seasonal pattern in both health-care systems. Adult vomiting-related calls to LHH (Figure 2) and to THC (Figure 2) showed increases during November and December. Pediatric diarrhea calls to LHH showed a major increase from October to December each year (Figure 2), whereas calls to THC peaked from February to May (Figure 2). Respiratory conditions peaked in the winter, and skin rashes peaked in the summer (not shown).
The diarrheal disease outbreak in Milwaukee (first noticed by a pharmacist on April 1, 1993 [7], and reported by the Milwaukee Health Department on April 7 [11]), was the largest reported waterborne outbreak in U.S. history, affecting almost half the city's population. Nurse hot line data showed an increase in diarrhea-related calls on April 2, a day after the pharmacist noted an increase in antidiarrhea drug sales and 5 days before the health department reported the outbreak. Media exposure on April 4 did not affect the initial increase detected by hot line data but may have affected the peak on April 10. The hot lines detected an increase in diarrhea even though almost all the callers lived in neighborhoods least affected by the outbreak. Since hot lines serve the areas in which they are located, no citywide analysis of disease patterns was possible.
The collection of hot line data was passive, but because reports came regularly, no data were missed. Unlike systems monitoring school absenteeism or nursing home illnesses, nurse hot lines provide symptom-based illness reports. Although they do not identify specific pathogens, hot line calls can provide a sentinel of increased illnesses for various conditions, including diarrhea, vomiting, and respiratory illness. Information on symptoms can be obtained rapidly.
The dramatic increase in the number of hot line calls during the Milwaukee cryptosporidiosis outbreak indicates that call volume may prospectively identify an outbreak. If hot lines serve a large area, they could also provide geographic information on the populations affected. As use of hot line data becomes more established, better estimates of expected daily and monthly variation in call volume should emerge, making detection of excess illness easier. Analysis of another outbreak may confirm the results of our study. However, a survey of state public health epidemiology programs found that no state uses or plans to use nurse hot line information for disease surveillance (12). With the decline in resources for state disease surveillance programs (13), nurse hot lines can inexpensively enhance existing surveillance programs.
Jane S. Rodman, postdoctoral research associate, Southwest Center for Managed Care Research, Albuquerque, New Mexico, has conducted research on cell biology structure and function and serologic surveillance of infectious diseases. Her areas of expertise include cell biology methods, Cryptosporidium, and viral serology tools.
Acknowledgment
The research described in this article has been supported by the U.S. Environmental Protection Agency through assistance agreement CR 824227 to The Lovelace Institutes.
References
- Kirner JC, Littler JD, Angelo LA. A waterborne outbreak of giardiasis in Camas, Wash. J Am Water Works Assoc. 1978;70:35–40.
- Foster LR. Surveillance for waterborne illness and disease reporting: state and local responsibilities. In: Craun GF, editor. Methods for the investigation and prevention of waterborne disease outbreaks. Washington: U.S. EPA Office of Research and Development; 1990. Report No.: EPA/600/1-90/005a.
- Karalekas PC, Taylor FB. Regulations and surveillance. In: Craun GF, editor. Waterborne diseases in the United States. Boca Raton (FL): CRC Press; 1986.
- Goldstein ST, Juranek DD, Ravenholt O, Hightower AW, Martin DG, Mesnik JL, Cryptosporidiosis: an outbreak associated with drinking water despite state-of-the-art water treatment. Ann Intern Med. 1996;124:459–68.PubMedGoogle Scholar
- Leland D, McAnulty J, Keene W, Sterens G. A cryptosporidiosis outbreak in a filtered-water supply. J Am Water Works Assoc. 1993;85:34–42.
- Frost FJ, Craun CF, Calderon RL. Waterborne disease surveillance. J Am Water Works Assoc. 1996;88:66–78.
- Rodman JS, Frost F, Davis-Burchat L, Fraser D, Langer J, Jakubowski W. Pharmaceutical sales a method of disease surveillance. J Environ Health. 1997;60:8–14.
- Papzian R. Hold the phone. Harv Health Lett. 1992;18:1–3.
- Glasoper A, McGrath K. Telephone triage: extending practice. Nurs Stand. 1993;7:34–6.
- Curran CR. An interview with Sandra C. Matherly and Shannon Hodges. Nurs Econ. 1995;3:125–8.
- MacKenzie WR, Hoxie JN, Proctor ME, Gradus MS, Blair KA, Peterson DE, A massive outbreak in Milwaukee of cryptosporidium infection transmitted through the public water supply. N Engl J Med. 1994;331:161–7. DOIPubMedGoogle Scholar
- Frost FJ, Calderon RL, Craun GL. Waterborne disease surveillance: findings of a survey of state and territorial epidemiology programs. J Environ Health. 1995;58:6–11.
- Berkelman RL, Bryan RT, Osterholm MT, LeDuc JW, Hughes JM. Infectious disease surveillance: a crumbling foundation. Science. 1994;264:368–70. DOIPubMedGoogle Scholar
Figures
Cite This ArticleTable of Contents – Volume 4, Number 2—June 1998
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Floyd Frost, Southwest Center for Managed Care Research, 2425 Ridgecrest Drive SE, Albuquerque, NM 87108, USA; fax: 505-262-7043
Top