Volume 13, Number 11—November 2007
Dispatch
Human Multidrug-Resistant Salmonella Newport Infections, Wisconsin, 2003–2005
Cite This Article
Citation for Media
Abstract
We conducted a retrospective study of Salmonella Newport infections among Wisconsin residents during 2003–2005. Multidrug resistance prevalence was substantially greater in Wisconsin than elsewhere in the United States. Persons with multidrug-resistant infections were more likely than persons with susceptible infections to report exposure to cattle, farms, and unpasteurized milk.
During the past decade, multidrug-resistant (MDR) Salmonella enterica serotype Newport strains in the United States have increased substantially (1). The prevalence of the most common MDR S. Newport phenotype, Newport-MDRAmpC, increased from 1% of human S. Newport isolates tested in 1998 to 21% of isolates tested in 2003 (2). Newport-MDRAmpC is resistant to at least chloramphenicol, streptomycin, sulfamethoxazole/sulfisoxazole, tetracycline, amoxicillin-clavulanic acid, ampicillin, cefoxitin, ceftiofur, and cephalothin. This phenotype exhibits decreased susceptibility to ceftriaxone (2), a critically important antimicrobial agent for treating invasive salmonellosis in children (3).
Studies suggest that dairy cattle are a major US reservoir for MDR S. Newport (4–6). However, data documenting the prevalence of MDR S. Newport among infected human case-patients in dairy-intensive states are limited. To assess the prevalence of resistance among S. Newport isolates in Wisconsin, which in 2002 had the greatest density of milk cows in the United States (7), we evaluated antimicrobial susceptibility data from S. Newport infections among Wisconsin case-patients during 2003–2005. We also compared information on potential exposures for case-patients with Newport-MDRAmpC and susceptible infections.
Surveillance data were electronically compiled for laboratory-confirmed S. Newport infections among Wisconsin residents with illness onsets from January 1, 2003, through December 31, 2005. Providers and local health departments reported hospitalization status; travel history; and exposure to raw milk, cattle, horses, reptiles, and dead animals. The study population included case-patients whose isolates were tested for antimicrobial drug susceptibility at the Wisconsin State Laboratory of Hygiene. Identification and susceptibility testing were conducted on isolates from stool, urine, and blood samples.
Serotype identification was performed according to the Kauffmann-White scheme (8). Slide and tube agglutination were used for identification of O (somatic) and H (flagellar) antigens, respectively. All isolates were tested for susceptibility to ampicillin, amoxicillin-clavulanic acid, cefoxitin, ceftriaxone, cephalothin, chloramphenicol, ciprofloxacin, gentamicin, kanamycin, nalidixic acid, streptomycin, sulfisoxazole, tetracycline, and trimethoprim-sulfamethoxazole, by using the Kirby-Bauer disk diffusion method. Results were interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines (9). Antimicrobial agents were categorized into CLSI antimicrobial subclasses, and each isolate was assigned to >1 categories according to its antimicrobial resistance phenotype and the number of subclasses to which it was resistant (National Antimicrobial Resistance Monitoring System for Enteric Bacteria [NARMS], pers. comm.; Table 1). Pansusceptible isolates were defined as isolates that had no detected antimicrobial drug resistance. Because isolates were not tested for ceftiofur resistance, our definition of Newport-MDRAmpC did not include resistance to this drug.
The prevalence of each type of resistance among S. Newport isolates from Wisconsin case-patients was compared with that reported elsewhere in the United States, by using 2003 and preliminary 2004 NARMS data. Data were analyzed by using Epi Info 2002, version 3.3.2 (Centers for Disease Control and Prevention, Atlanta, GA, USA); to assess associations between antimicrobial resistance and reported exposures, odds ratios and Mantel-Haenszel and Fisher exact 2-tailed p values were calculated where appropriate.
Figure
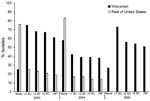
Figure. Antimicrobial drug resistance patterns of human Salmonella Newport isolates from Wisconsin (2003–2005) and elsewhere in the United States (2003–2004), based on data provided by the National Antimicrobial Resistance Monitoring System for...
Serotyping and antimicrobial drug susceptibility testing were conducted on S. Newport isolates from 268 case-patients. Median age was 34 years (range <1–96 years); of 267 case-patients for whom sex was reported, 57% were female. Resistance patterns are provided in Table 1. Among the 5 (2%) quinolone-resistant isolates (2 resistant to nalidixic acid and ciprofloxacin, 2 resistant to nalidixic acid only, and 1 resistant to ciprofloxacin only), 4 were ceftriaxone resistant and 1 was MDRAmpC resistant. The frequencies of antimicrobial drug resistance among Wisconsin S. Newport isolates were substantially greater for all resistance subgroups than frequencies reported elsewhere in the United States during 2003 and 2004 (NARMS, pers. comm.; Table 1; Figure).
Of 194 case-patients for whom hospitalization status was reported, 46 (24%) had been hospitalized. Of case-patients with Newport-MDRAmpC and pansusceptible infections, similar proportions were hospitalized (26% and 24%, respectively) and had known hospitalization status (72% and 73%, respectively). Two case-patients died: an 84-year-old woman and a 37-year-old man for whom salmonellosis was not considered the probable cause of death. The 2 associated isolates were pansusceptible.
Persons infected with Newport-MDRAmpC were significantly more likely than persons infected with pansusceptible S. Newport to be male and to have had contact with cattle, to have drunk unpasteurized milk, and to live on or have visited a farm or petting zoo (Table 2). Reported exposure to reptiles was significantly associated with pansusceptible infection (Table 2). No association was found between hospitalization and resistance (odds ratio [OR] 1.09, p = 0.81).
We describe a substantially greater prevalence of MDRAmpC resistance among Wisconsin case-patients with S. Newport infections that occurred during 2003–2005, compared with data reported elsewhere in the United States (NARMS, personal communication, 2007). This finding is of particular concern because Newport-MDRAmpC exhibits decreased susceptibility to ceftriaxone, a third-generation cephalosporin that is the treatment of choice for invasive salmonellosis in children (3). Additionally, because the blaCMY-2 gene that confers ceftriaxone resistance in Newport-MDRAmpC is located on a plasmid that was readily transferred between Escherichia coli in laboratory assays (10), propagation of Newport-MDRAmpC could increase the spread of CMY-2 plasmids to other bacteria.
Patients with Newport-MDRAmpC infection were more likely than patients with pansusceptible infections to report contact with cattle, farms, and unpasteurized milk. These exposures are likely to be more common among patients with Newport-MDRAmpC infection than among the general Wisconsin population, which suggests that dairy cattle are an important reservoir for Newport-MDRAmpC. Increased prevalence of Newport-MDRAmpC in Wisconsin may be due to selective pressure from the use of antimicrobial drugs on dairy farms (1), particularly ceftiofur, an extended-generation cephalosporin closely related to ceftriaxone (which is commonly used in cattle) (11). Clonally and independently acquired CMY-2–associated ceftiofur resistance has been identified among Salmonella strains isolated from dairy farms (12).
Few published data are available on the prevalence of Newport-MDRAmpC in other dairy-intensive states. Minnesota, which in 2002 had the eighth-greatest density of milk cows in the United States (7), reported a significant increase in MDR S. Newport among human isolates during 1996–2003, including an increase in the percentage of isolates with decreased susceptibility to ceftriaxone (13). However, NARMS reported a similar increase in Newport-MDRAmpC prevalence nationally during 1998–2003 (2). Analyses of unpublished data provided by the Minnesota Department of Health indicated that 22% of 147 human isolates tested had antimicrobial drug resistance profiles consistent with the Newport-MDRAmpC phenotype during 2003–2005; this prevalence is much lower than that among Wisconsin case-patients who were ill during the same period. Although differences in enteric disease surveillance could partially explain this discrepancy, Newport-MDRAmpC’s emergence in dairy cattle is likely to be associated with several factors.
Our findings underscore the need for intensive Newport-MDRAmpC surveillance in major dairy states. Efforts to promote the conservative and appropriate use of ceftiofur and other antimicrobial drugs in dairy cattle are indicated; they should be complemented by strategies to discourage transmission of MDR Salmonella among cattle, such as separating ill from parturient animals and disinfecting environmental niches (14). Furthermore, providers should be discouraged from prescribing antimicrobial drugs to patients with low-risk Salmonella infections (15), and public health messages should emphasize the importance of pasteurizing milk and cooking meat appropriately.
Dr Karon is an Epidemic Intelligence Service Officer at the Centers for Disease Control and Prevention. Her research interests include emerging zoonoses, antimicrobial resistance, and food safety.
Acknowledgment
We are grateful to NARMS for providing data on S. Newport resistance patterns for the United States excluding Wisconsin. We also thank Stephanie Wedel and Fe Leano for providing unpublished data from Minnesota, and Jeffrey P. Davis for assistance with manuscript preparation.
References
- Gupta A, Fontana J, Crowe C, Bolstorff B, Stout A, Van Duyne A, Emergence of multidrug-resistant Salmonella enterica serotype Newport infections resistant to expanded-spectrum cephalosporins in the United States. J Infect Dis. 2003;188:1707–16. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. National Antimicrobial Resistance Monitoring System for Enteric Bacteria (NARMS): 2003 human isolates final report. Atlanta: US Department of Health and Human Services, the Centers; 2006.
- Guerrant RL, Van Gilder T, Steiner TS, Thielman NM, Slutsker L, Tauxe RV, Practice guidelines for the management of infectious diarrhea. Clin Infect Dis. 2001;32:331–51. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Outbreak of multidrug-resistant Salmonella Newport—United States, January–April 2002. MMWR Morb Mortal Wkly Rep. 2002;51:545–8.PubMedGoogle Scholar
- Rankin SC, Aceto H, Cassidy J, Holt J, Young S, Love B, Molecular characterization of cephalosporin-resistant Salmonella enterica serotype Newport isolates from animals in Pennsylvania. J Clin Microbiol. 2002;40:4679–84. DOIPubMedGoogle Scholar
- Varma JK, Marcus R, Stenzel SA, Hanna SS, Gettner S, Anderson BJ, Highly resistant Salmonella Newport-MDRAmpC transmitted through the domestic US food supply: a FoodNet case-control study of sporadic Salmonella Newport infections, 2002–2003. J Infect Dis. 2006;194:222–30. DOIPubMedGoogle Scholar
- United States Department of Agriculture. 2002 census of agriculture–volume 1 geographic area series census, US—state data [cited 2007 Feb 26]. Available from http://www.nass.usda.gov/Census/Create_Census_US.jsp#top.
- Centers for Disease Control and Prevention. Salmonella Surveillance Summary, 2002 [cited 2007 Aug 20]. Atlanta: US Department of Health and Human Services, The Centers, 2003. Available from http://www.cdc.gov/NCIDOD/DBMD/phlisdata/salmtab/2002/SalmonellaIntroduction2002
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing; sixteenth informational supplement, M100–S16. Wayne (PA): The Institute; 2006.
- Winokur PL, Vonstein DL, Hoffman LJ, Uhlenhopp EK, Doern GV. Evidence for transfer of CMY-2 AmpC beta-lactamase plasmids between Escherichia coli and Salmonella isolates from food animals and humans. Antimicrob Agents Chemother. 2001;45:2716–22. DOIPubMedGoogle Scholar
- Zwald AG, Ruegg PL, Kaneene JB, Warnick LD, Wells SJ, Fossler C, Management practices and reported antimicrobial usage on conventional and organic dairy farms. J Dairy Sci. 2004;87:191–201. DOIPubMedGoogle Scholar
- Alcaine SD, Sukhnanand SS, Warnick LD, Su WL, McGann P, McDonough P, Ceftiofur-resistant Salmonella strains isolated from dairy farms represent multiple widely distributed subtypes that evolved by independent horizontal gene transfer. Antimicrob Agents Chemother. 2005;49:4061–7. DOIPubMedGoogle Scholar
- Lopes VC, Wedel SD, Bender JB, Smith KE, Leano FT, Boxrud DJ, Emergence of multidrug-resistant Salmonella enterica serovar Newport in Minnesota. Clin Infect Dis. 2006;43:210–3. DOIPubMedGoogle Scholar
- Cobbold RN, Rice DH, Davis MA, Besser TE, Hancock DD. Long-term persistence of multidrug-resistance Salmonella enterica serovar Newport in two dairy herds. J Am Vet Med Assoc. 2006;228:585–91. DOIPubMedGoogle Scholar
- Devasia RA, Varma JK, Whichard J, Gettner S, Cronquist AB, Hurd S, Antimicrobial use and outcomes in patients with multi-drug resistant and pansusceptible Salmonella Newport infections, 2002–2003. Microb Drug Resist. 2005;11:371–7. DOIPubMedGoogle Scholar
Figure
Tables
Cite This ArticleTable of Contents – Volume 13, Number 11—November 2007
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Amy E. Karon, PO Box 5452, Hercules, CA 95457, USA:
Top