Volume 13, Number 5—May 2007
Research
Respirator Donning in Post-Hurricane New Orleans
Cite This Article
Citation for Media
Abstract
We evaluated correctness of N95 filtering facepiece respirator donning by the public in post-hurricane New Orleans, where respirators were recommended for mold remediation. We randomly selected, interviewed, and observed 538 participants, using multiple logistic regression for analysis. Only 129 (24%) participants demonstrated proper donning. Errors included nose clip not tightened (71%) and straps incorrectly placed (52%); 22% put on the respirator upside down. Factors independently associated with proper donning were as follows: ever having used a mask or respirator (odds ratio [OR] 5.28; 95% confidence interval [CI], 1.79–22.64); ever having had a respirator fit test (OR 4.40; 95% CI, 2.52–7.81); being male (OR 2.44; 95% CI, 1.50–4.03); Caucasian race (OR 2.09; 95% CI, 1.32–3.33); having a certified respirator (OR 1.99, 95% CI 1.20–3.28); and having participated in mold clean-up (OR 1.82; 95% CI,1.00–3.41). Interventions to improve respirator donning should be considered in planning for influenza epidemics and disasters.
Figure 1
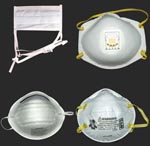
Figure 1. Noncertified masks and certified respirators. A surgical mask (upper left) and a dust mask (lower left) are examples of disposable masks that are not designed to filter small particles and that...
Many respirators certified by the National Institute for Occupational Safety and Health (NIOSH), particularly disposable N95 filtering facepiece respirators (N95 FF respirators [Figure 1]), are available to the public. The certification indicates that the respirator material will perform at a given filter efficiency (1). Because proper fit is also necessary for respirator function, US regulations state that an employer who requires workers to wear respirators must establish a respiratory protection program that covers respirator selection and maintenance, fit testing, and worker instruction (2). Although nonoccupational respirator use has not been well studied, members of the public who use respirators may be less likely than workers in a respiratory protection program to achieve a proper fit, given lack of formal training (3).
Public health agencies have recommended N95 FF respirators to members of the public for some situations. Such occasions have included after major floods, for potential heavy exposure to bioaerosols in water-damaged buildings (Grand Forks, North Dakota, 1997; eastern North Carolina after Hurricane Floyd, 1999) (4), and for settings that pose a risk for airborne transmission of infection, such as during the severe acute respiratory syndrome (SARS) epidemic (for select patients at risk of acquiring the infection and for persons visiting patients with SARS) (5–7). There is also a longstanding recommendation for N95 FF respirator use for visitors of hospitalized patients with tuberculosis (8). The US Department of Health and Human Services (HHS) currently recommends that persons living in or visiting an area affected by avian influenza A (H5N1) wear N95 FF respirators when in contact with birds in an enclosed environment (9).
In the fall of 2005, after the unprecedented flooding in New Orleans, Louisiana caused by Hurricanes Katrina and Rita, public health officials recommended that members of the public use N95 FF respirators when cleaning or remediating mold-contaminated buildings (10). A survey of 159 New Orleans area residents 7 weeks after Katrina found that 68% of those interviewed were aware of the recommendation (11) and that at least 30% of those participating in remediation activities had used a NIOSH-certified respirator (12). Despite these levels of awareness and experience, subsequent anecdotal reports suggested that some New Orleans residents were not properly donning N95 FF respirators. Improper donning would promote the entry of unfiltered air through leaks or gaps between the respirator and the skin, compromising the protection offered (13). To better understand respirator use by the public, we investigated the nonoccupational use and donning of N95 FF respirators in post-hurricane New Orleans.
Participants
Using geographic information system mapping software, we randomly selected homes in Orleans Parish (city of New Orleans). To focus on residential areas, we eliminated 6,345 of the parish’s 10,181 census blocks (US Census, 2000). The eliminated blocks were likely to be sparsely populated or to contain industrial buildings, commercial centers, or parks (blocks with <20 housing units and blocks in the lower 2.5% of housing unit density); to contain mostly high-rise apartment buildings or public housing units that would be difficult to access or remain uninhabited (blocks in the upper 2.5% of housing unit density); and to be in uninhabited neighborhoods (blocks in the Lower Ninth Ward). We randomly generated 600 waypoints (unique locations based on latitude and longitude) across the remaining 3,836 census blocks.
Each waypoint served as a starting point to locate eligible participants. Using a global positioning system device, a survey team navigated to a waypoint and identified the nearest home. To be eligible for participation, a person had to be an English-speaking adult (>18 years of age) associated with a home as its owner, current occupant, or relative/friend of the owner/occupant. Because we were interested in nonoccupational respirator use by the general public, persons at a home as paid employees (e.g., remediators) were not eligible. However, residents encountered at their own homes who were employed as remediators were not excluded. If unable to conduct an interview at the first encountered home, the team proceeded in a systematic fashion to the next home. Once 1 interview was conducted at a waypoint, the team navigated to the next waypoint and repeated the process.
Questionnaire and Evaluation of Respirator Donning
From March 4 to March 11, 2006, survey team members interviewed participants with a 10-minute questionnaire that collected information on experience with residential flooding, water damage, and mold growth; participation in mold clean-up activities; lifetime and post-Katrina experiences with respiratory protection (both noncertified dust masks and surgical masks, hereafter “masks”; and NIOSH-certified respirators, including disposable and reusable types, hereafter “certified respirators”); and nonidentifying demographic factors, including self-identified ethnicity and race. Each team used the same photographs and actual examples of masks and certified respirators during the interviews.
Figure 2

Figure 2. Properly donned disposable N95 filtering facepiece respirator. To be properly donned, the respirator must be correctly oriented on the face and held in position with both straps. The straps must be...
Each interview included an evaluation of respirator donning. Interviewers were trained before the survey on proper donning (Figure 2), including the following: proper orientation of the respirator; use of both straps; proper placement of straps; need for tightening of the nose clip; and need for removal of facial hair (14,15). A participant with an N95 FF respirator that appeared to be in good condition was permitted to use this respirator for the evaluation. Otherwise, the participant was asked to choose between 2 models then available from New Orleans retailers. The interviewer asked the participant to put on the N95 FF respirator as he or she would for participating in mold clean-up activities. Written and pictorial manufacturer’s instructions were included with the respirator packaging, but no additional instructions were given until the evaluation was complete (16). The interviewer recorded whether the participant referred to the manufacturer’s instructions and, once the participant indicated that the respirator was donned, noted any observed “donning errors” that could contribute to an insufficient fit.
Statistical Analyses
For calculations of frequencies of donning errors, we included all participants who had at least 1 error. However, because 2 errors, visible gap and facial hair, could reflect aspects of study design (size and shape of respirators offered and lack of opportunity to shave before evaluation, respectively) rather than participants’ donning technique, they were not considered in analyses of factors associated with proper donning. For these analyses, participants with at least 1 of the other donning errors were categorized as improperly donning the respirator; the remaining participants were categorized as properly donning the respirator.
To identify factors associated with proper donning, we used contingency tables and simple logistic regression. We included significant factors (p<0.05) in multiple logistic regression models, applying stepwise logistic regression. We used the likelihood ratio χ2 test and calculated odds ratios (OR) with 95% likelihood confidence intervals (CI). We conducted analyses with SAS (version 9.1) and JMP (version 5.1) software packages (SAS Institute, Cary, NC, USA).
Participants
We conducted 553 interviews at the 600 visited waypoints, for a response rate of 92%. Half of the participants were male, with a median age of 50 years, and about half identified their race as Caucasian and half as African-American or black (Table 1). Most described previously using a mask or respirator, but few reported ever having a respirator fit test. Most had participated in mold clean-up activities since Hurricane Katrina.
Respiratory Protection Use during Mold Clean-up Activities
Overall, of the 553 participants interviewed, 42% (n = 233) had used a certified respirator, and 35% (n = 192) had used an N95 FF respirator, specifically, for mold clean-up activities since Katrina. Among the 368 who reported participating in mold clean-up activities, most (n = 315, 86%) reported using a mask or certified respirator during those activities, most frequently the N95 FF respirator (Table 2). A minority (n = 60, 19%) of the 315 reported referring to the manufacturer’s instructions. More commonly (n = 129, 41%), participants stated that they used respiratory protection without any instruction.
Evaluation of Respirator Donning
A total of 538 (97%) participants agreed to put on an N95 FF respirator. Most of these (n = 489, 91%) used 1 of the 2 models offered by the interviewers. Twelve (2%) referred to the manufacturer’s directions.
Overall, 433 (80%) of the participants who donned an N95 FF respirator were noted to have at least 1 donning error that could contribute to a poor fit. More than half of these did not tighten the nose clip, and half incorrectly placed the 2 straps; in addition, 22% put the respirator on upside down, and 21% used only 1 strap (Table 3). While 31% (n = 135) made l error, 34% (n = 146) made 2, and 35% (n = 152) made >3.
Characteristics Associated with Proper Donning
For 24 participants, the only noted donning error was a visible gap (n = 6) or facial hair (n = 18). When these 24 persons who otherwise demonstrated proper donning were included, 129 (24%) of the participants properly donned the N95 FF respirator. In simple logistic regression analyses of all participants, proper donning was significantly associated with several personal factors: being male, being Caucasian, and being a nonrenter (i.e., a homeowner or associate) in the home at which the interview occurred. In addition, proper donning was associated with post-hurricane experiences: having been inside a water-damaged or moldy home and having participated in mold clean-up. Finally, proper donning was associated with several factors related to respirators: ever having used a mask or certified respirator, ever having had a respirator fit test, having at the time of the interview a mask or certified respirator, and having at the time of the interview a respirator confirmed by the interviewer to be NIOSH certified (Table 4).
For the subset that had participated in clean-up activities, proper donning was also associated with use of respiratory protection during clean-up, including having specifically used an N95 FF respirator. For the subset that had used a mask or certified respirator during clean-up, having obtained that mask or respirator from the workplace and having obtained information on how to use the mask or respirator from the workplace were also significant factors. Proper donning was not associated with age, Hispanic ethnicity, level of floodwater, water incursion due to roof or window damage, extent of mold coverage, current employment in mold remediation, asthma diagnosis, smoking status, or respirator brand.
When multiple logistic regression was used, the factors significantly associated with proper donning for all participants were as follows: ever having used a mask or certified respirator (OR 5.28; 95% CI, 1.79–22.64), ever having had a respirator fit test (OR 4.40; 95% CI, 2.52–7.81), being male (OR 2.44; 95% CI, 1.50–4.03), being Caucasian (OR 2.09; 95% CI, 1.32–3.33), having a certified respirator at the time of the interview (OR 1.99, 95% CI 1.20–3.28), and having participated in mold clean-up activities (OR 1.82; 95% CI,1.00–3.41). For the subset that participated in mold clean-up, the significant factors were as follows: having used a certified respirator during clean-up (OR 5.17; 95% CI, 2.75–10.24); ever having had a respirator fit test (OR 3.38; 95% CI, 1.75–6.61); being Caucasian (OR 3.38, 95% CI, 1.97–5.91); and being male (OR 2.80; 95% CI, 1.58–5.13). These same factors were also significant for the subset that used a mask or certified respirator during clean-up.
The protection afforded by a certified respirator depends on its fit, and a fundamental component of achieving a good fit is proper donning (13,17). In post-hurricane New Orleans, public concern about adverse health effects of exposure to mold was near universal (11,12). Yet our investigation demonstrated that, despite this high level of motivation, most of participants did not properly don an N95 FF respirator.
Our investigation benefited from several strengths. We used a random selection process to obtain our sample, and comparisons with existing population-based surveys suggest we achieved a representative cross-section (18,19). Given inconsistencies in respiratory protection terminology, we facilitated effective communication by using photographs and actual examples of masks and certified respirators. Finally, of the few prior field investigations that have addressed N95 FF respirator donning (20–22), none have focused on nonoccupational use.
An important limitation is that we did not confirm the observed proper donnings with respirator fit testing. While we cannot estimate the relative contribution of each donning error to declining protection without quantitative measurements, those participants who put on the respirator improperly would clearly have failed a standard fit test. However, the outcome in those who appeared to properly put on the respirator is less certain because even a properly donned respirator may have leaks that limit its effectiveness. A study of 18 different N95 FF respirator models found that, overall, in the absence of fit testing, 74% of proper donnings would provide the full protection possible with an N95 FF respirator (range 31%–99%, depending on the model) (23). Thus, the proportion of our participants who would have achieved the full protection possible with an N95 FF respirator is likely to be lower than the proportion who demonstrated proper donning. Ultimately, designing models with good fit characteristics would be beneficial.
Our findings have implications for the use of N95 FF respirators by members of the public to prevent the transmission of communicable diseases. Both experimental and epidemiologic studies suggest that airborne transmission of influenza (by small particles <10 μm) can occur and may result in more severe disease than transmission by large droplets or fomites (24–27). A recent review argues that airborne transmission may play an important role in the spread of a pandemic strain (28). While formal recommendations for N95 FF respirator use by the public do not exist—beyond the HHS recommendation regarding potential exposures to infected birds—a recent Institute of Medicine (IOM) report notes that “a properly fitted N95 FF respirator is likely to be both the least expensive and the most widely available NIOSH-certified respirator for protecting... the public against airborne [influenza] infection” (29). Our results suggest that much of the public may have difficulty achieving a proper fit because of improper donning. Given the observed role of experience in proper donning, and the high frequency of recent experience with respirators reported by our survey participants, one could argue that the overall performance in post-Katrina New Orleans is likely to be superior to that of virtually any other locale.
The World Health Organization anticipates use of respiratory protection by the public will occur spontaneously in the event of pandemic influenza (30,31). Indeed, N95 FF respirators are currently being marketed to the public as “bird flu masks” (32). While uncertainty remains about the level of protection needed against influenza and that offered by an N95 FF respirator, an improperly donned N95 FF respirator will provide less protection than a properly donned one. Our results suggesting that workplace training increased proper donning among the public indicate that educational efforts could have a positive effect. Since few of our participants reported, or were observed, referring to manufacturers’ instructions, consideration also should be given to incorporating instructions onto the respirator itself, such as arrows or simple words (“nose,” “chin”) to indicate orientation. The IOM report’s authors could find no simple modification of N95 FF respirators that would prevent the need for fit testing (29). Short of mass fit testing, proper donning will be the vital step to ensuring that members of the public using N95 FF respirators derive the greatest possible benefit from them.
Even under workplace conditions, respirator donning may be imperfect. An observational study of 62 healthcare workers in 3 California hospitals found that 40 (65%) improperly put on N95 FF respirators before entering the room of a patient in isolation for tuberculosis. Errors included use of only 1 strap, incorrectly placed straps, and presence of facial hair (21). The results of that study, in terms of the proportion who demonstrated improper donning and the nature of the errors, are similar to our findings. The impact of the 2005 US policy that suspended enforcement of annual fit testing of healthcare workers who use respirators for occupational exposure to tuberculosis is unknown (33). Yet N95 FF respirators will clearly be part of healthcare workers’ defense in the event of pandemic influenza (34,35). HHS, as part of procurement of essential medical supplies for pandemic influenza, has stockpiled 20 million N95 FF respirators and plans to acquire 87 million more through September 2007 (36). The pandemic plans of other countries, including Australia and France, recommend use of N95 (or FFP2) respirators (28). Further evaluation of respirator donning among healthcare workers therefore may be warranted.
In summary, this population-based survey of nonoccupational respirator use found that a minority of participants demonstrated proper donning of an N95 FF respirator. Our findings are of particular importance to public health agencies planning for future events, from floods to pandemic influenza, in which use of N95 FF respirators by the public will be recommended or is anticipated. A unique opportunity exists to enhance protection of the public through interventions, such as educational campaigns, training sessions, and respirator design modifications, aimed at improving the public’s ability to don a respirator correctly. Infection control officers and the healthcare workers they protect also may benefit from the insights gained from this survey.
Dr Cummings is an Epidemic Intelligence Service Officer with the Centers for Disease Control and Prevention and NIOSH. Her research interests include respiratory infections and their prevention.
Acknowledgments
We thank the following people for their assistance: Roland J. Berry Ann, Jr., Chris Coffey, Bill Miller, John R. Myers, and Raoult Ratard for their contributions to design; Kathleen B. Fedan for her assistance with design and interviewer training; Beth A. Ramage for her assistance with interviewer training; Steven R. Game for his contributions to design, interviewer training, and data acquisition; Hannah Alsdurf, Michael Beaty, Brent C. Doney, Matthew Duling, Monica C. Graziani, Mark F. Greskevitch, Todd C. Noletto, Amy M. Nuernberg, David L. Spainhour, James E. Taylor, Brian D. Tift, and Snigdha Vallabhaneni for their roles in data acquisition; and Gerald R. Hobbs for his contribution to data analysis.
This investigation was supported by intramural funding provided by the Division of Respiratory Disease Studies, NIOSH, Morgantown, West Virginia; the National Personal Protective Technology Laboratory, NIOSH, Pittsburgh, Pennsylvania; and the Office of Workforce and Career Development, Centers for Disease Control and Prevention, Atlanta, Georgia.
References
- United States Department of Health and Human Services. National Institute for Occupational Safety and Health. 42 CFR Part 84. [cited 2006 Dec 8]. Available from http://www.cdc.gov/niosh/part84.txt
- United States Department of Labor. Occupational Health and Safety Administration. Regulations (Standards 29 CFR): Respiratory protection–1910.134. [cited 2006 Dec 8]. Available from http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=12716&p_table=STANDARDS
- Hannum D, Cycan K, Jones L, Stewart M, Morris S, Markowitz SM, The effect of respirator training on the ability of healthcare workers to pass a qualitative fit test. Infect Control Hosp Epidemiol. 1996;17:636–40.PubMedGoogle Scholar
- National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. HETA 99–0363 final report. Cincinnati (OH): The Institute; 1999.
- Kao TW, Huang KC, Huang YL, Tsai TJ, Hsieh BS, Wu MS. The physiological impact of wearing an N95 mask during hemodialysis as a precaution against SARS in patients with end-stage renal disease. J Formos Med Assoc. 2004;103:624–8.PubMedGoogle Scholar
- Chaovavanich A, Wongsawat J, Dowell SF, Inthong Y, Sangsajja C, Sanguanwongse N, Early containment of severe acute respiratory syndrome (SARS); experience from Bamrasnaradura Institute, Thailand. J Med Assoc Thai. 2004;87:1182–7.PubMedGoogle Scholar
- World Health Organization. Hospital infection control guidance for severe acute respiratory syndrome (SARS). April 2003. [cited 2006 Dec 8]. Available from http://www.who.int/csr/sars/infectioncontrol/en
- Centers for Disease Control and Prevention. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Morb Mortal Wkly Rep. 2005;54(RR-17):1–141.PubMedGoogle Scholar
- United States Department of Health and Human Services. Pandemicflu.gov questions and answers. [cited 2006 Dec 8]. Available from http://answers.pandemicflu.gov
- Centers for Disease Control and Prevention. Mold prevention strategies and possible health effects in the aftermath of hurricanes and major floods. MMWR Morb Mortal Wkly Rep. 2006;55(RR-8):1–27.PubMedGoogle Scholar
- Centers for Disease Control and Prevention. Health concerns associated with mold in water-damaged homes after hurricanes Katrina and Rita—New Orleans area, Louisiana, October 2005. MMWR Morb Mortal Wkly Rep. 2006;55:41–4.PubMedGoogle Scholar
- Cummings KJ, Van Sickle D, Rao CY, Riggs MA, Brown C, Moolenaar RL. Mold-related knowledge, attitudes, and practices of residents and remediation workers in post-hurricane New Orleans. Arch Environ Occup Health. 2006;61. In press. DOIPubMedGoogle Scholar
- Crutchfield CD, Fairbank EO, Greenstein SL. Effect of test exercises and mask donning on measured respirator fit. Appl Occup Environ Hyg. 1999;14:827–37. DOIPubMedGoogle Scholar
- Skretvedt OT, Loschiavo JG. Effect of facial hair on the face seal of negative-pressure respirators. Am Ind Hyg Assoc J. 1984;45:63–6. DOIPubMedGoogle Scholar
- Stobbe TJ, daRoza RA, Watkins MA. Facial hair and respirator fit: a review of the literature. Am Ind Hyg Assoc J. 1988;49:199–204. DOIPubMedGoogle Scholar
- 3M. Example of manufacturer’s instructions for use of disposable N95 FF respirator. [cited 2006 Dec 8]. Available from http://multimedia.mmm.com/mws/mediawebserver.dyn?6666660Zjcf6lVs6EVs666vQFCOrrrrQ-
- Campbell DL, Coffey CC, Jensen PA, Zhuang Z. Reducing respirator fit test errors: a multi-donning approach. J Occup Environ Hyg. 2005;2:391–9. DOIPubMedGoogle Scholar
- City of New Orleans. Emergency Operations Center. Rapid Population Estimate Project, January 28–29, 2006 survey report. [cited 2006 Nov 2]. Available from http://katrina.lsu.edu/downloads/research/NOLAPopEstimate.pdf
- Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion. Behavioral Risk Factor Surveillance System. [cited 2006 Dec 8]. Available from http://www.cdc.gov/brfss/index.htm
- Stricof RL, Delles LP, Difernando G Jr. Mask/particulate respirator use by employees at risk for exposure to multi-drug resistant tuberculosis. Am J Respir Crit Care Med. 1994;149(Suppl):A855.
- Sutton PM, Nicas M, Harrison RJ. Tuberculosis isolation: comparison of written procedures and actual practices in three California hospitals. Infect Control Hosp Epidemiol. 2000;21:28–32. DOIPubMedGoogle Scholar
- Biscotto CR, Pedroso ER, Starling CE, Roth VR. Evaluation of N95 respirator use as a tuberculosis control measure in a resource-limited setting. Int J Tuberc Lung Dis. 2005;9:545–9.PubMedGoogle Scholar
- Coffey CC, Lawrence RB, Campbell DL, Zhuang Z, Calvert CA, Jensen PA. Fitting characteristics of eighteen N95 filtering-facepiece respirators. J Occup Environ Hyg. 2004;1:262–71. DOIPubMedGoogle Scholar
- Schulman JL. Experimental transmission of influenza virus infection in mice. IV. Relationship of transmissibility of different strains of virus and recovery of airborne virus in the environment of infector mice. J Exp Med. 1967;125:479–88. DOIPubMedGoogle Scholar
- Moser MR, Bender TR, Margolis HS, Noble GR, Kendal AP, Ritter DG. An outbreak of influenza aboard a commercial airliner. Am J Epidemiol. 1979;110:1–6.PubMedGoogle Scholar
- Alford RH, Kasel JA, Gerone PJ, Knight V. Human influenza resulting from aerosol inhalation. Proc Soc Exp Biol Med. 1966;122:800–4.PubMedGoogle Scholar
- Bridges CB, Kuehnert MJ, Hall CB. Transmission of influenza: implications for control in health care settings. Clin Infect Dis. 2003;37:1094–101. DOIPubMedGoogle Scholar
- Tellier R. Review of aerosol transmission of influenza A virus. Emerg Infect Dis. 2006 Nov. [cited 2006 Dec 8]. Available from https://wwwnc.cdc.gov/eid/article/12/11/06-0426_article
- Institute of Medicine. Reusability of facemasks during an influenza pandemic: facing the flu. Washington: The National Academies Press; 2006.
- World Health Organization. Non-pharmaceutical interventions: their role in reducing transmission and spread. [cited 2006 Dec 8]. Available from http://www.col.ops-oms.org/servicios/influenza/reunion/docs/WHO_intervenciones_no_farmacologicas.pdf
- World Health Organization Writing Group. Nonpharmaceutical interventions for pandemic influenza, national and community measures. Emerg Infect Dis. 2006 Jan. [cited 2006 Dec 8]. Available from https://wwwnc.cdc.gov/eid/article/12/1/05-1371_article
- Example of website marketing N95 FF respirators as “bird flu masks.” [cited 2006 Dec 8]. Available from http://www.bestbirdflumasks.com
- United States Department Labor. Occupational Health and Safety Administration. Tuberculosis and respiratory protection: prohibition of enforcing annual fit testing requirements during 2005 fiscal year; enforcement of other 1910.134 provisions. Dec 22, 2004. [cited 2006 Dec 8]. Available from http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=24977
- Centers for Disease Control and Prevention. Interim recommendations for infection control in health-care facilities caring for patients with known or suspected avian influenza. [cited 2006 Dec 8]. Available from http://www.cdc.gov/flu/avian/professional/infect-control.htm
- World Health Organization. WHO global influenza preparedness plan. [cited 2006 Dec 8]. Available from http://www.who.int/csr/resources/publications/influenza/GIP_2005_5Eweb.pdf
- United States Department of Health and Human Services. Pandemic planning update II, June 29, 2006. [cited 2006 Dec 8]. Available from http://www.pandemicflu.gov/plan/pdf/PanfluReport2.pdf
Figures
Tables
Cite This ArticleTable of Contents – Volume 13, Number 5—May 2007
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Kristin J. Cummings, NIOSH, 1095 Willowdale Rd, Mailstop 2800, Morgantown, WV 26505, USA;
Top