Volume 14, Number 3—March 2008
Dispatch
Screening Pneumonia Patients for Mimivirus1
Cite This Article
Citation for Media
Abstract
Acanthamoeba polyphaga mimivirus (APM), a virus of free-living amebae, has reportedly caused human respiratory disease. Using 2 newly developed real-time PCR assays, we screened 496 respiratory specimens from 9 pneumonia-patient populations for APM. This virus was not detected in any specimen, which suggests it is not a common respiratory pathogen.
Investigation of a suspected Legionnaire’s pneumonia outbreak in 1992 led to the isolation of a new microorganism from a water cooling tower in Bradford, England. This pathogen was thought to be a bacterium because it resembled small gram-positive cocci; however, in 2003 it was correctly identified as a virus (1). Acanthamoeba polyphaga mimivirus (APM), named for its ameba host and bacteria-mimicking characteristics, is a double-stranded DNA virus with the largest viral genome described to date (1.2 Mb) (2). Mimiviridae is the newest member of the nucleocytoplasmic large DNA virus (NCLDV) group, which also contains Poxviridae, Iridoviridae, Asfarviridae, and Phycodnaviridae (1). APM encodes specific translation proteins that are more commonly associated with cellular organisms than with viruses (2).
Other ameba-associated microorganisms from environmental sources, such as Legionella pneumophila, are known to cause outbreaks of acute pneumonia in immunosuppressed and elderly persons, although person-to-person transmission is uncommon. Whether APM is similarly responsible for individual cases or outbreaks of respiratory disease has yet to be conclusively determined. Previous studies have reported serologic evidence of APM infection in 7.1% to 9.7% of patients with community- or nosocomially acquired pneumonia (3,4). APM DNA was also amplified by a nested PCR assay from a bronchoalveolar lavage specimen of a 60-year-old patient receiving intensive care for hospital-acquired pneumonia (3). In this study, we used newly developed real-time PCR assays to screen pneumonia patients from a variety of epidemiologic settings for APM infections.
Real-time PCR assays for APM were developed from multiple primers and probes designed for conserved regions of class I NCLDV genes L396 and R596, class III NCLDV gene L65, as well as the R656 gene, from the published APM genome sequence (GenBank accession no. NC_006450) by using Primer Express 3.0 software (Applied Biosystems, Foster City, CA, USA). All probes were labeled at the 5′ end with 6-carboxy-fluorescein and quenched at the 3′ end with Black Hole Quencher-1 (Biosearch Technologies, Novato, CA, USA). Different primer and probe combinations were evaluated, and the 2 PCR assays that gave the best performance were selected for further studies (Table 1). Assays were performed by using the iQSupermix Kit (Bio-Rad, Hercules, CA, USA) in 25-μL reaction volumes. Amplification was performed on an iCycler iQReal-Time Detection System (Bio-Rad) by using the following cycling conditions: 95ºC for 3 min for 1 cycle; 95ºC for 15 s and 55ºC for 1 min for 45 cycles each. Total nucleic acid was extracted from all specimens by using either the NucliSens Automated Extractor (bioMérieux, Boxtel, the Netherlands) or the automated BioRobot MDx (QIAGEN, Valencia, CA, USA) according to the manufacturers’ instructions. Each clinical specimen was also tested for the human ribonuclease P gene to measure nucleic acid integrity as previously described (5).
For PCR-positive controls, recombinant plasmids containing APM DNA (kindly provided by Didier Raoult, Unite des Rickettsies, Universite de la Mediterranee, Marseille, France) were constructed. Primer pairs bracketing the L396 and R596 genes were used to amplify 1,560-bp and 879-bp full gene regions, respectively, using 300 nmol/L of forward primers 396 F (5′-TTA ATC ATC TTC CAA AAA ATT TAA TTC-3′) and 596 F (5′-ATG TCG TTA TCA AAA CAA GTA GTT CC-3′), and 300 nmol/L of reverse primers 396 R (5′-ATG GCG AAC AAT ATT AAA ACT AAA A-3′) and 596 R (5′-CTA ATT TTC AAT ATA GTG CGT AGA TTC TA-3′). These PCR products were purified by using the QIAquick Gel Extraction Kit (QIAGEN) and then cloned into a pCR-II TOPO vector by using a TOPO TA Cloning Kit (Invitrogen, Carlsbad, CA, USA). Recombinant plasmids were then isolated by using the QIAprep Spin Miniprep Kit (QIAGEN) and quantified by UV spectroscopy. Standard curves were prepared from serial 10-fold dilutions of the quantified plasmid in nuclease-free water containing 100 μg/mL of herring sperm DNA (Promega, Madison, WI, USA).
Figure 1
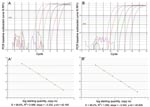
Figure 1. Real-time PCR amplification plots and standard curves for Acanthamoeba polyphaga mimivirus (APM)-396 (A, A′) and APM-596 (B, B’). Linear amplification was achieved over 6 logs for both assays over 5 ×...
The L396 and R596 real-time PCR assays could detect as few as 10 copies of plasmid DNA per reaction with amplification efficiencies of 99.6% [slope –3.33 and r2 = 0.99] (Figure 1, left panels) and 99.2% [slope –3.34 and r2 = 1.00] (Figure 1, right panels), respectively. No amplification was obtained by either assay with pooled total nucleic acid extracts from respiratory samples from healthy humans or from other common DNA respiratory viruses, including adenovirus, human bocavirus, or herpesviruses.
The real-time PCR assays were used to test respiratory specimens from 496 pneumonia cases representing 9 distinct patient populations, which consisted of hospitalized pneumonia patients from population-based pneumonia surveillance studies in Thailand and the United States, transplant recipients with pneumonia, and isolated pneumonia outbreaks in either retirement homes for the elderly or familial clusters (Table 2). Of the 496 specimens tested, no positive results were obtained for APM DNA by either assay.
We developed a rapid method of screening samples for APM DNA by using 2 sensitive and specific real-time PCR assays designed to target conserved NCLDV class I genes. With only 1 APM sequence published (NC_006450) (2), little is known of APM strain variation; therefore, use of assays that target different genes increases the likelihood that genetic variants of APM will not be missed. A suicide-nested PCR method for APM detection has been reported (3); however, the quicker turnaround time and lower risk for amplicon contamination makes the real-time PCR method more attractive for screening large numbers of samples.
A seroprevalence study of APM among Canadian patients with community-acquired pneumonia identified APM antibodies in 9.7% of 376 patients compared with 2.3% of 511 healthy controls (3). However, seropositivity may reflect exposure to APM antigen rather than active infection, and the potential for nonspecific cross-reactions with the serologic assays used may have inflated the true prevalence of APM infection (6). In a separate report, a laboratory-acquired APM infection was linked to acute pneumonia by seroconversion in a technician in Marseille, France, thus providing evidence that this virus can occasionally cause clinical disease (7). However, using sensitive real-time PCR assays, we failed to detect APM DNA in 496 respiratory specimens from 9 epidemiologically varied pneumonia patient populations.
If we assume an APM prevalence of 0.2% (1 case in the study sample), the estimated probability of obtaining our results by chance, based on binomial analysis, would be 0.37. Most of the specimens we tested were from the upper respiratory tract, whereas the only reported APM PCR–positive sample was from a lower respiratory bronchoalveolar lavage specimen (3). Moreover, the patient populations sampled may not represent those at highest risk for APM infection. Nevertheless, our study supports the findings of an Austrian study that failed to detect APM in 214 nasopharyngeal specimens from hospitalized children with respiratory symptoms (8).
Our study did not detect APM in a large collection of specimens from patients with pneumonia, which indicates that this virus is not a common cause of severe acute respiratory disease. Because APM is an ameba-associated pathogen like Legionella, exposures to APM are most likely to occur from environmental sources. Further studies of more epidemiologically appropriate populations may be necessary to adequately access the importance of APM as a potential human respiratory pathogen. The real-time PCR assays described here will help facilitate these studies.
Mr Dare is a microbiologist in the Division of Viral Diseases at the Centers for Disease Control and Prevention. His research focuses on developing molecular diagnostic assays for respiratory viruses.
References
- Scola B, Audic S, Robert C, Jungang L, Lamballerie X, Drancourt M, A giant virus in amoebae. Science. 2003;299:2033. DOIPubMedGoogle Scholar
- Raoult D, Audic S, Robert C, Abergal C, Renesto P, Ogata H, The 1.2-megabase genome sequence of mimivirus. Science. 2004;306:1344–50. DOIPubMedGoogle Scholar
- La Scola B, Marrie TJ, Auffray JP, Raoult D. Mimivirus in pneumonia patients. Emerg Infect Dis. 2005;11:449–52.PubMedGoogle Scholar
- Berger P, Papazian L, Drancourt M, La Scola B, Auffray JP, Raoult D. Ameba-associated microorganisms and diagnosis of nosocomial pneumonia. Emerg Infect Dis. 2006;12:248–55.PubMedGoogle Scholar
- Emery SL, Erdman DD, Bowen MD, Newman BR, Winchell JM, Meyer RF, Real-time reverse transcription-polymerase chain reaction assay for SARS-associated coronavirus. Emerg Infect Dis. 2004;10:311–6.PubMedGoogle Scholar
- 6. Raoult D, La Scola B, Birtles R. The discovery and characterization of mimivirus, the largest known virus and putative pneumonia agent. Clin Infect Dis. 2007;45:95–102. DOIPubMedGoogle Scholar
- Raoult D, Renesto P, Brouqui P. Laboratory infection of a technician by mimivirus. Ann Intern Med. 2006;144:702–3.PubMedGoogle Scholar
- Larcher C, Jeller V, Fischer H, Huemer P. Prevalence of respiratory viruses, including newly identified viruses, in hospitalized children in Austria. Eur J Clin Microbiol Infect Dis. 2006;25:681–6. DOIPubMedGoogle Scholar
Figure
Tables
Cite This Article1Dare et al., Acanthamoeba polyphaga mimivirus real-time PCR assays, was presented at the 23rd Annual Clinical Virology Symposium, Apr 29–May 2, 2007, in Clearwater Beach, Florida, USA.
Table of Contents – Volume 14, Number 3—March 2008
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Dean D. Erdman, Centers for Disease Control and Prevention, Mailstop G04, 1600 Clifton Rd NE, Atlanta, GA 30333, USA;
Top