Volume 17, Number 2—February 2011
Dispatch
Comparison of Pandemic (H1N1) 2009 and Seasonal Influenza Viral Loads, Singapore
Cite This Article
Citation for Media
Abstract
Mean viral loads for patients with pandemic (H1N1) 2009 were ≈1 log10 times lower than those for patients with seasonal influenza within the first week after symptom onset. Neither pandemic nor seasonal influenza viral loads correlated with clinical severity of illness. No correlation was found between viral loads and concurrent illness.
Although clinical characteristics of pandemic (H1N1) 2009 have been well documented (1,2), fewer specific virologic comparisons with seasonal influenza have been studied in hospitalized patients (3). Studies of other influenza virus infections in humans suggest that host immune responses play a major role in determining clinical outcomes (4,5). We describe the initial viral loads for patients infected with pandemic (H1N1) 2009 and seasonal (H1 and H3) influenza viruses and their correlation with various aspects of signs and symptoms at admission to the National University Hospital (NUH) in Singapore.
The study consisted of patients seen at NUH during May–November 2009 as emergency admissions, outpatients, or inpatients whose nasopharyngeal swabs submitted for routine diagnostic testing were positive for seasonal influenza virus A (H1 and H3) or pandemic influenza A virus (H1N1) 2009. From samples taken before treatment was begun, we identified 578 patients with pandemic (H1N1) 2009 and 88 patients with seasonal influenza (11 H1 and 77 H3). Clinical characteristics of some of these patients have been described elsewhere (2). Local ethics approval (ref. no. B/09/360) was granted for this study.
Age, sex, and clinical information (i.e., days after onset of symptoms, comorbidities, clinical severity) were obtained from patient records. Comorbidities were defined as >1 of the conditions listed in Table 1. Clinical severity was defined as follows: mild, patients well enough to be treated as outpatients; moderate, patients ill enough to warrant hospital admission; severe, hospitalized patients who died or who required intensive or high-dependency care. In-house quantitative assays (Technical Appendix) were performed on archived samples previously tested as positive for pandemic (H1N1) 2009 and reported elsewhere (6).
Figure 1
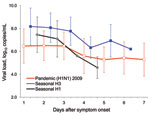
Figure 1. Viral loads (in RNA copies/mL) in patients with pandemic (H1N1) 2009 (NP) and seasonal H1 and H3 (MP) influenza at time patient sought hospital care against days after symptom onset. Vertical...
Viral loads of hemagglutinin (HA) and nucleoprotein (NP) for pandemic (H1N1) 2009 ranged from 102 to 109 RNA copies/mL of virus transport medium (mean 105–107 RNA copies/mL). Seasonal influenza viral loads ranged from 103 to 1010 RNA copies/mL (mean 106–108 RNA copies/mL for seasonal influenza subtype H3 and mean 105 to 107 RNA copies/mL for seasonal influenza H1). Viral loads decreased with time after onset of symptoms from date the patient sought care at NUH in patients with pandemic or seasonal influenza (Figure 1).
Because of the small number of patients with seasonal influenza H1, further analysis for seasonal influenza was limited to H3. Patients infected with pandemic (H1N1) 2009, compared with those having seasonal influenza H3, were younger (p<0.0001), and a higher proportion had comorbidities (p = 0.0068; Table 1).
Figure 2

Figure 2. A) Profile plot and multivariate comparisons of the estimated nucleoprotein viral loads of pandemic (H1N1) 2009, by patient age group, against days from symptom onset in the final multiple analysis of...
For the 578 pandemic influenza cases, the multiple analysis of variance showed that viral loads were associated with number of days after symptom onset from date of presentation (p<0.0001) and with age (p = 0.0112) (Figure 2, panel A; Table 2). For the 77 seasonal influenza H3 cases, the analysis of variance showed that days after onset of symptoms from date of presentation (p = 0.0223) and presence of any comorbidities (p = 0.0249) significantly affected viral loads (Table 2). Viral loads for seasonal influenza were lower in patients with than without comorbidities (Figure 2, panel B).
One of our most striking findings was that the mean viral loads of patients visiting NUH were ≈1 log10 higher for seasonal than for pandemic influenza (Figure 1). This difference persisted even after we adjusted for age. Another study demonstrated that within the first 3 days after symptom onset, historical mean viral loads of seasonal influenza exceed those of the contemporary pandemic virus by 1–2 log10 (3). However, a limitation of that study is its use of viral load data for seasonal influenza that was historical rather than obtained contemporaneously with the data for pandemic (H1N1) 2009.
Approximately 30%–50% of influenza case-patients may be asymptomatic (7), and although the correlation between viral load and clinical symptoms is not well established, a viral load threshold may exist below which most persons have no clinical symptoms (although individual variation will always exist). Our analysis suggests that if such a threshold exists, it is lower for novel than for seasonal influenza viruses. For a direct virus-mediated pathologic process, this hypothesis may be understandable, given the lower prevalence of preexisting (and therefore potentially partially protective) cross-reactive immunity for this novel virus (8–10).
Viral loads for both pandemic (H1N1) 2009 and seasonal influenza tend to decrease with time after symptom onset (Figure 1). Larger studies are needed to confirm the more rapid decline of seasonal influenza H1 than of H3 viral loads. In addition, younger age groups had significantly higher viral loads for pandemic (H1N1) 2009 (Figure 2, panel A), which may not be surprising given that this Southeast Asian population appears to have little or no preexisting specific or cross-reacting antibodies to this novel virus (9,10).
Two findings are perhaps the most surprising of this analysis. First, we found no significant correlation between pandemic (H1N1) 2009 or seasonal influenza viral loads and clinical severity of illness (Table 2). Second, pandemic (H1N1) 2009 viral loads in infected patients with and without preexisting comorbidities did not differ significantly, although a significant difference was found for seasonal influenza (Figure 2, panel B; Table 2). We offer some possible explanation for these findings but note that these influenza viral loads have been measured in respiratory samples. These samples are peripheral types of specimens that may not necessarily directly affect, or be directly affected by, many of the preexisting comorbidities that involve nonrespiratory systems, unless their management involves, for example, some sort of immunosuppressive therapy.
A main limitation of this study is that these viral load measurements were performed on only 1 acute diagnostic sample from each patient at admission before treatment with oseltamivir; therefore, determining how these viral loads would have changed later during the natural course of the infection was not possible. Also, some of the patient categories (Table 1, Table 2) contained relatively few patients, e.g., the relatively low number of severe cases (Table 1, Table 2), which may have limited the statistical significance of some correlations. Finally, although influenza viral loads in various types of respiratory samples are now often reported (3,6), these are heterogeneous, peripheral samples, and such viral loads may vary considerably in the same patient during a single day, depending on individual host immune responses.
If human illness caused by influenza virus infections is mediated by host immune responses (4,5), then a more vigorous, primary immune response in the immunologically naive, otherwise healthy younger population against the pandemic (H1N1) 2009 virus may also contribute to the degree of clinical illness. The interplay between a direct viral pathologic process and a host immune-mediated pathologic process is probably unique to each person. Some recent studies investigating cytokine responses in persons with acute pandemic (H1N1) 2009 infections had contrasting findings (11–13), although postmortem investigations of some fatal cases of pandemic (H1N1) 2009 infection found substantial inflammation, which supports an immune-mediated pathologic process for at least in these cases (14). Similarly, for the more well-established seasonal H3 influenza (to which most persons have had many years of exposure) more well-established, robust, yet sufficiently individually different patterns of homologous and heterologous immune responses may contribute more (compared with similar responses to pandemic [H1N1] 2009) to the different degrees of clinical illness in infected persons with different combinations of comorbidities.
Dr Chun K. Lee is a member of the diagnostic and research team at the Molecular Diagnosis Centre at the National University Hospital in Singapore. His main research interest is developing and validating molecular assays for clinical and research applications in infectious diseases and detecting human genetic and metabolic disorders.
Acknowledgment
P.A.T. was supported by the Asia Pacific Influenza Advisory Committee and MerLion Pharma; lecture fees from Pfizer, Novartis, Wyeth, and International Business Communications Asia; and grant support from Baxter, Interimmune, and Adamas.
References
- Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team; Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, . Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009;360:2605–15.DOIGoogle Scholar
- Tang JW, Tambyah PA, Lai FY, Lee HK, Lee CK, Loh TP, Differing symptom patterns in early pandemic vs seasonal influenza infections. Arch Intern Med. 2010;170:861–7.DOIGoogle Scholar
- To KK, Chan KH, Li IW, Tsang TY, Tse H, Chan JF, Viral load in patients infected with pandemic H1N1 2009 influenza A virus. J Med Virol. 2010;82:1–7.DOIGoogle Scholar
- Peiris JS, Cheung CY, Leung CY, Nicholls JM. Innate immune responses to influenza A H5N1: friend or foe? Trends Immunol. 2009;30:574–84.DOIGoogle Scholar
- Kobasa D, Jones SM, Shinya K, Kash JC, Copps J, Ebihara H, Aberrant innate immune response in lethal infection of macaques with the 1918 influenza virus. Nature. 2007;445:319–23.DOIGoogle Scholar
- Lee HK, Lee CK, Loh TP, Tang JW, Chiu L, Tambyah PA, Diagnostic testing for pandemic influenza in Singapore: a novel dual-gene quantitative real-time RT-PCR for the detection of influenza A/H1N1/2009. J Mol Diagn. 2010;12:636–43.DOIGoogle Scholar
- Bridges CB, Kuehnert MJ, Hall CB. Transmission of influenza: implications for control in health care settings. Clin Infect Dis. 2003;37:1094–101.DOIGoogle Scholar
- Hancock K, Veguilla V, Lu X, Zhong W, Butler EN, Sun H, Cross-reactive antibody responses to the 2009 pandemic H1N1 influenza virus. N Engl J Med. 2009;361:1945–52.DOIGoogle Scholar
- Chen H, Wang Y, Liu W, Zhang J, Dong B, Fan X, Serologic survey of pandemic (H1N1) 2009 virus, Guanxi Province, China. Emerg Infect Dis. 2009;15:1849–50.
- Tang JW, Tambyah PA, Wilder-Smith A, Puong KY, Shaw R, Barr IG, Cross-reactive antibodies to pandemic (H1N1) 2009 virus, Singapore. Emerg Infect Dis. 2010;16:874–6.
- Woo PC, Tung ET, Chan KH, Lau CC, Lau SK, Yuen KY. Cytokine profiles induced by the novel swine-origin influenza A/H1N1 virus: implications for treatment strategies. J Infect Dis. 2010;201:346–53.DOIGoogle Scholar
- Bermejo-Martin JF, Ortiz de Lejarazu R, Pumarola T, Rello J, Almansa R, Ramirez P, Th1 and Th17 hypercytokinemia as early host response signature in severe pandemic influenza. Crit Care. 2009;13:R201.DOIGoogle Scholar
- Bermejo-Martin JF, Martin-Loeches I, Rello J, Antón A, Almansa R, Xu L, Host adaptive immunity deficiency in severe pandemic influenza. Crit Care. 2010;14:R167.DOIGoogle Scholar
- Gill JR, Sheng Z-M, Ely SF, Guinee DG, Beasley MB, Suh J, Pulmonary pathologic findings of fatal 2009 pandemic influenza A/H1N1 viral infections. Arch Pathol Lab Med. 2010;134:235–43.
Figures
Tables
Cite This ArticleTable of Contents – Volume 17, Number 2—February 2011
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Julian W Tang, Department of Laboratory Medicine, National University Hospital, 5 Lower Kent Ridge Rd, Singapore 119074
Top