Volume 20, Number 10—October 2014
Online Report
Dengue Expansion in Africa—Not Recognized or Not Happening?
Suggested citation for this article
Abstract
An expert conference on Dengue in Africa was held in Accra, Ghana, in February 2013 to consider key questions regarding the possible expansion of dengue in Africa. Four key action points were highlighted to advance our understanding of the epidemiology of dengue in Africa. First, dengue diagnostic tools must be made more widely available in the healthcare setting in Africa. Second, representative data need to be collected across Africa to uncover the true burden of dengue. Third, established networks should collaborate to produce these types of data. Fourth, policy needs to be informed so the necessary steps can be taken to provide dengue vector control and health services.
Approximately 2.5–4 billion persons, 40%–60% of the world’s population, live in areas at risk for dengue virus (DENV) infection (1,2). With an estimated annual total of 390 million infections, dengue is the most frequent mosquito-borne viral disease worldwide (3). However, it is a neglected tropical disease (4), which might be the situation in Africa.
Since 1960, evidence of DENV transmission has been documented in 32 countries in Africa (5). The global share of apparent infections believed to occur in Africa (≈16% of 96 million infections worldwide) is of the same order of magnitude as that for Latin America (≈14%) (3). However, more limited occurrence data for Africa (3) and less consensus on the presence of DENV transmission in many countries in Africa (2) indicate that burden predictions remain uncertain.
With the recent growing global interest in dengue, the number of diagnostically robust reports from Africa has increased. All 4 DENV serotypes have now been documented to circulate in Africa, although DENV-2 has been reported most frequently (6). In 2010, DENV-3 outbreaks were reported in Tanzania, Zanzibar, the Comoros, Benin, and Cape Verde (7–9), followed by reports during 2011–2013 of substantial numbers of cases in Angola (10), Kenya (11), and Somalia (Centers for Disease Control and Prevention, unpub. data) caused by DENV-1. Preliminary phylogenetic studies indicate that the DENV-1 strain isolated in Angola clustered with strains from Côte d’Ivoire (1985, 1998, and 1999) and Nigeria (1968), which suggested transmission of endemic strains of DENV-1 in Africa (12). Case reports of returning travelers (7,13,14), and sequence data from sylvatic DENV strains (15,16) account for most of what is known at the genomic level regarding DENV circulating in Africa.
Unprecedented human mobility, rapid urban population growth, and large-scale changes in ecosystems have been associated with an increase in dengue transmission in Latin America and Asia, and are likely to favor spread of DENV into new locations (17–20). Reasons for an apparent emergence of DENV in Africa might include increased awareness of the disease, availability of better diagnostic tests, and improved access to specialized laboratory facilities. However, the range and lack of specificity of the symptoms of dengue indicate that clinical diagnosis is often difficult, even in dengue-endemic areas, where the index of suspicion is high among health care workers. Thus, hidden among the many febrile illnesses in Africa (malarial, bacterial, viral, rickettsial), dengue could have been overlooked, and the conspicuous mismatch between estimated disease incidence and actual number of reported cases might reflect a failure to consider dengue in the differential diagnosis of these common conditions.
In contrast, the clinical features of severe dengue are more distinct, although only a small fraction of DENV-infected patients progress to this stage (21). Until recently, severe dengue had been reported infrequently in Africa. However, among Ugandan peacekeepers deployed in Somalia, bleeding was reported in 12% of case-patients (Centers for Disease Control and Prevention, unpub. data). Six case-patients with severe dengue, including 1 who died (3% of 196 confirmed cases), were reported in an urban epidemic in Senegal in 2009 (22), and 11 deaths were reported in Luanda, Angola, in 2013 (23). Several possible reasons must be considered to explain why, if disease incidence across Africa is high, the severe end of the disease spectrum has not been more regularly detected. First, similar to the argument proposed earlier with respect to symptomatic dengue in general, clinicians unfamiliar with the disease may fail to consider the possibility of severe dengue in their differential diagnosis of patients with hypovolemic shock, severe bleeding, or severe organ dysfunction. Second, severe dengue occurs only rarely in Africa.
One hypothesis that has been proposed to support the rare occurrence of severe dengue in Africa suggests that protective genetic variants may be present in populations in Africa (24). The absence of recorded episodes of severe dengue in children in Haiti during 1994–1996, despite high transmission (25), and data for Cuba showing lower hospitalization rates for severe dengue among subpopulations of African ancestry (26–29), support this hypothesis. In addition, a study from Bahia, Brazil, assigned ancestry on the basis of genetic markers, and reported an association between African ancestry and a reduced risk for severe dengue (30). However, cases of severe dengue have been reported in the past from Africa (31–33), and illness and death from severe dengue have been documented during recent outbreaks when intensive surveillance was conducted.
An expert conference on Dengue in Africa was organized by the International Research Consortium on Dengue Risk Assessment, Management, and Surveillance (IDAMS) (European FP7; www.idams.eu) and the International Network for the Demographic Evaluation of Populations and Their Health (INDEPTH) (www.indepth-network.org) and held in Accra, Ghana, in February 2013 to consider key questions regarding dengue in Africa. Have we failed to observe an escalation of dengue in Africa causing a disease incidence of similar magnitude to that of Latin America, or is dengue truly not spreading into Africa for epidemiologic reasons that are not yet understood? The meeting addressed 4 major themes surrounding this central issue to advance our understanding of the epidemiology of dengue in Africa: 1) diagnostic tools and diagnostic capacity development; 2) improving estimates of the epidemiology and incidence of dengue; 3) biology of vectors and implications for vector control strategies; and 4) health policy, health services, and epidemic preparedness. The considerations and main suggestions for each theme are outlined in this report.
Figure
Diagnostic capacity for dengue, as for virtually all causes of acute febrile illness (AFI), is limited in Africa (34). However, there are reliable serologic assays for the diagnosis of acute dengue, which require only modest technologic expertise and investment in infrastructure (35–38). Several rapid tests with reasonable sensitivity and specificity are available (39–42). Deployment of point-of-care testing or ELISA-based serologic assay methods (IgM, IgG, and nonstructural protein 1) at sentinel sites where risk for dengue is estimated to be high, would support accurate diagnosis and potentially raise awareness of the disease locally. A wide range of more sophisticated diagnostics, including PCR for DENV RNA, plaque-reduction neutralization tests, or microneutralization tests, are also available and could be integrated into national and regional reference laboratories (Figure), along with appropriate capacity development.
Implementation of a tiered laboratory diagnostic system along these lines across Africa would facilitate unambiguous diagnosis of dengue infection in a subset of clinically suspected cases, provide quality assurance and quality control for feeder laboratories, and support a program of locally relevant scientific research. For example, 1 major step would be to evaluate these diagnostic tests in patients with AFI and take into account the high background endemicity of malaria and various co-circulating flaviviruses.
Africa lacks systematic surveillance and reporting of many diseases, including dengue (43). Information from archived serum samples from a variety of repositories retrospectively tested for acute DENV infection could be used to clarify the extent of transmission across Africa. This information includes studies of AFI, malaria, influenza-like illness, yellow fever, or measles-negative specimens in rash–illness studies. Prospective AFI studies are also needed to ascertain whether case definitions for dengue in Africa differ from those for Asia, the Americas, and Oceania.
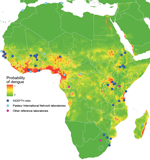
The African INDEPTH member sites provide a unique opportunity to conduct denominator-based research for more reliable quantification of the burden of dengue in Africa. The INDEPTH network includes 35 health and demographic surveillance systems (HDSSs) in Africa, which are producing longitudinal demographic data about lives of persons in low-income and middle-income countries (44). Prospective efforts to quantify the presence of dengue can be guided by existing reports, as well as by published risk maps (3). Analysis of climatic, demographic, and socioeconomic variables of precise locations where dengue has been reported in Africa enables generation of predictive models that can suggest other environments suitable for DENV transmission (Figure). These models can provide a basis for future hypothesis-driven research regarding the presence and quantification of dengue in Africa. Results of such research would, in return, improve the accuracy of subsequent risk maps. In addition, because molecular epidemiologic studies and phylogenetic analysis of DENV strains will provide more informed insight into origins and distribution of DENV across Africa, submission of sequence data for as many samples as possible should also be encouraged.
Should dengue be identified as imposing a major burden in Africa, it will be essential to understand the biology and behavior of local vectors because these factors will influence transmission, as well as selection and design of effective control tools and strategies. The 2 major DENV vectors (Aedes aegypti and Ae. albopictus mosquitoes) are present in Africa. In Senegal, other Aedes mosquito species have also been shown to be involved in transmission of sylvatic dengue (45).
At least 2 forms of Ae. aegypti mosquitoes need to be distinguished in Africa: an ancestral forest or sylvan form, and a global domestic form. These 2 forms differ in distribution, behavior (46,47), and potentially in vector competence for DENV (48). Additional genetic variability might be present within the global domestic form (49). Older studies have reported unusual bionomics, such as high levels of nocturnal bloodfeeding, exophily, or dispersal in Ae. aegypti mosquitoes in Africa (50,51).
Ae. albopictus mosquitoes continue to spread through Africa since they were first reported in Nigeria in 1991, and these mosquitoes might play a major role in the epidemiology of dengue in Africa (52). This vector was incriminated as the sole vector in a dengue outbreak in central Africa in 2007 (20). Recent studies in Cameroon reported Ae. albopictus mosquitoes blood-feeding on humans (53) and breeding in domestic water containers (54) at levels that exceed those seen outside Africa.
Dengue vector control requires thorough knowledge of vector biology and behavior to be effective (55). The effect of existing malaria vector control programs (targeted for anopheline species of mosquitoes) on DENV vectors is likely to be minimal because malaria control in Africa is typically conducted in rural settings, targeting the nocturnally active vectors inside homes with long-lasting insecticide-treated bed nets or in the large natural water bodies where breeding occurs. Conversely, Aedes spp. mosquitoes are diurnally active, which indicates that long-lasting insecticide-treated bed nets are ineffective for dengue vector control (17,55,56). These mosquitoes also breed in artificial containers in urban domestic environments, which makes management of rural water bodies equally irrelevant for dengue control. Spraying of insecticides in and around homes is a common approach for limiting dengue vector populations, but studies have not shown it to be an effective control strategy on its own (57).
Given a lack of awareness of dengue in Africa, it is perhaps not surprising that dengue control is a low-priority health policy in this region (3). DENV transmission in Asia and Latin America is concentrated around unplanned urban and semi-urban areas with poor infrastructure (18), a condition that is widespread and increasing in Africa (58,59). Dengue epidemics in densely populated areas regularly drive health facilities in Asia and Latin America to their limits (60). Therefore, health services in Africa should be prepared to face similar challenges, and this preparation relies crucially on collection of more and improved baseline epidemiologic data. These data are essential for monitoring trends of disease occurrence, identifying epidemic-prone areas, and assessing the potential benefits of a future dengue vaccine on burden reduction in the region (61).
In summary, the expert conference in Accra highlighted 4 key action points. First, dengue diagnostic tools must be made more widely available in the health care setting in Africa. Second, representative data need to be collected across Africa to uncover the true incidence of dengue and more clearly define its transmission in the region. Third, established networks, such as African laboratory networks, the Pasteur International network, the INDEPTH network, and others, should collaborate to produce these needed types of data. Fourth, policy needs to be informed by improved information to take necessary steps for dengue vector control and provision of health services. Addressing these issues will be essential before any major future decisions regarding control or prevention of dengue in Africa can be made.
Dr Jaenisch is a senior scientist at Heidelberg University Hospital, Heidelberg, Germany. His research interests are the epidemiology of infectious disease, especially dengue.
Acknowledgments
Members of the Dengue in Africa Study Group: Thierry A. Ouedraogo (Nouna HDSS, Burkina Faso); Oliver J. Brady, Andrew Farlow, Simon I. Hay, Janey P. Messina, (Oxford University, Oxford, UK); Isabella Eckerle (University of Bonn Medical Centre, Bonn, Germany); Moses Gwamaka (Rufiji HDSS, Tanzania); Thomas Jaenisch, Thomas Junghanss (Heidelberg University Hospital, Heidelberg, Germany); Harold S. Margolis (Centers for Disease Control and Prevention, San Juan, Puerto Rico, USA); Philip J. McCall (Liverpool School of Tropical Medicine, Liverpool, UK); Abraham Oduro (Navrongo HDSS, Ghana); Victor Ofula (US Army Medical Research Unit–Kenya, Nairobi, Kenya); Osman Sankoh (INDEPTH Network, Accra, Ghana and University of the Witwatersrand, Johannesburg, South Africa); Anavaj Sakunthabhai (Institut Pasteur, Paris, France); Amadou A. Sall (Institut Pasteur, Dakar, Senegal); Herrmann Sorgho (Nanoro HDSS, Burkina Faso); Alfred Tiono (Sapone HDSS, Burkina Faso); Raman Velayudhan (World Health Organization, Geneva); Bridget Wills (Oxford University Clinical Research Unit, Ho Chi Minh City, Vietnam); G.R. William Wint (Environmental Research Group Limited, Oxford, UK); Hervé Zeller (European Centre for Disease Control and Prevention, Stockholm, Sweden).
We thank the INDEPTH Secretariat for hosting the conference. This report is catalogued with the publication reference no. IDAMS23 (www.idams.eu).
The expert conference on dengue in Africa in Accra, Ghana, was supported by European Union grant FP7-281803 IDAMS.
References
- World Health Organization. Dengue and severe dengue. Fact sheet # 117, 2012 [cited 2014 Jul 21]. http://www.who.int/mediacentre/factsheets/fs117/en/
- Brady OJ, Gething PW, Bhatt S, Messina JP, Brownstein JS, Hoen AG, Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis. 2012;6:e1760. . Epub 2012 Aug 7.DOIGoogle Scholar
- Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, The global distribution and burden of dengue. Nature. 2013;496:504–7 . DOIGoogle Scholar
- World Health Organization. 17 neglected tropical diseases [cited 2014 Jul 21]. http://www.who.int/neglected_diseases/diseases/en/
- Amarasinghe A, Kuritsk JN, Letson GW, Margolis HS. Dengue virus infection in Africa. Emerg Infect Dis. 2011;17:1349–54 .PubMedGoogle Scholar
- Messina JP, Brady OJ, Scott TW, Zou C, Pigott DM, Duda KA, Global spread of dengue virus types: mapping the 70 year history. Trends Microbiol. 2014;22:138–46 . DOIPubMedGoogle Scholar
- Gautret P, Simon F, Hervius AH, Bouchaud O, Leparc-Goffart I, Ninove L, Dengue type 3 virus infections in European travellers returning from the Comoros and Zanzibar, February–April 2010. Euro Surveill. 2010;15:19541 .PubMedGoogle Scholar
- Gautret P, Botelho-Nevers E, Charrel RN, Parola P. Dengue virus infections in travellers returning from Benin to France, July–August 2010. Euro Surveill. 2010;15:19657 .PubMedGoogle Scholar
- Franco L, Di CA, Carletti F, Vapalahti O, Renaudat C, Zeller H, Recent expansion of dengue virus serotype 3 in west Africa. Euro Surveill. 2010;15:19490 .PubMedGoogle Scholar
- Centers for Disease Control and Prevention. Ongoing dengue epidemic—Angola, June 2013. MMWR Morb Mortal Wkly Rep. 2013;62:504–7 .PubMedGoogle Scholar
- PROMED. Dengue/DHF update (33): Asia, Africa, Pacific - (2) Kenya (Mombasa). PROMEDmail; 2013 Apr 28. Report No.: 20130428.1676860 [cited 2014 Jul 23]. http://www.promedmail.org
- Sessions OM, Khan K, Hou Y, Meltzer E, Quam M, Schwartz E, Exploring the origin and potential for spread of the 2013 dengue outbreak in Luanda, Angola. Glob Health Action. 2013;6:21822.PubMedGoogle Scholar
- Moi ML, Takasaki T, Kotaki A, Tajima S, Lim CK, Sakamoto M, Importation of dengue virus type 3 to Japan from Tanzania and Côte d’Ivoire. Emerg Infect Dis. 2010;16:1770–2 . DOIPubMedGoogle Scholar
- Wichmann O, Stark K, Shu PY, Niedrig M, Frank C, Huang JH, Clinical features and pitfalls in the laboratory diagnosis of dengue in travellers. BMC Infect Dis. 2006;6:120 . DOIPubMedGoogle Scholar
- Franco L, Palacios G, Martinez JA, Vazquez A, Savji N, De OF, First report of sylvatic DENV-2-associated dengue hemorrhagic fever in west Africa. PLoS Negl Trop Dis. 2011;5:e1251 . DOIPubMedGoogle Scholar
- Vasilakis N, Cardosa J, Hanley KA, Holmes EC, Weaver SC. Fever from the forest: prospects for the continued emergence of sylvatic dengue virus and its impact on public health. Nat Rev Microbiol. 2011;9:532–41 . DOIPubMedGoogle Scholar
- Anders KL, Hay SI. Lessons from malaria control to help meet the rising challenge of dengue. Lancet Infect Dis. 2012;12:977–84 . DOIPubMedGoogle Scholar
- Gubler DJ. Dengue, urbanization and globalization: the unholy trinity of the 21(st) century. Trop Med Health. 2011;39(Suppl):3–11 . DOIPubMedGoogle Scholar
- Higa Y. Dengue vectors and their spatial distribution. Trop Med Health. 2011;39(Suppl):17–27 . DOIPubMedGoogle Scholar
- Paupy C, Ollomo B, Kamgang B, Moutailler S, Rousset D, Demanou M, Comparative role of Aedes albopictus and Aedes aegypti in the emergence of dengue and chikungunya in central Africa. Vector Borne Zoonotic Dis. 2010;10:259–66 . DOIPubMedGoogle Scholar
- Simmons CP, Farrar JJ, Nguyen V, Wills B. Dengue. N Engl J Med. 2012;366:1423–32 . DOIPubMedGoogle Scholar
- Faye O, Ba Y, Faye O, Talla C, Diallo D, Chen R, Urban epidemic of dengue virus serotype 3 infection, Senegal, 2009. Emerg Infect Dis. 2014;20:456–9 . DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Dengue in Angola. 2013 [cited 2014 Jul 21]. http://wwwnc.cdc.gov/travel/notices/watch/dengue-angola
- de la C Sierra B. Kourí G, Guzman MG. Race: a risk factor for dengue hemorrhagic fever. Arch Virol. 2007;152:533–42 and.PubMedGoogle Scholar
- Halstead SB, Streit TG, Lafontant JG, Putvatana R, Russell K, Sun W, Haiti: absence of dengue hemorrhagic fever despite hyperendemic dengue virus transmission. Am J Trop Med Hyg. 2001;65:180–3 .PubMedGoogle Scholar
- Bravo JR, Guzman MG, Kouri GP. Why dengue haemorrhagic fever in Cuba? 1. Individual risk factors for dengue haemorrhagic fever/dengue shock syndrome (DHF/DSS). Trans R Soc Trop Med Hyg. 1987;81:816–20 . DOIPubMedGoogle Scholar
- González D, Castro OE, Kouri G, Perez J, Martinez E, Vazquez S, Classical dengue hemorrhagic fever resulting from two dengue infections spaced 20 years or more apart: Havana, Dengue 3 epidemic, 2001–2002. Int J Infect Dis. 2005;9:280–5 . DOIPubMedGoogle Scholar
- Guzman MG, Kouri GP, Vasquez S, Rosario D, Bravo JR, Valdez L. DHF Epidemics in Cuba, 1981 and 1997: some interesting observations. Dengue Bull. 1999;23:39–43.
- Morier L, Kouri G, Guzman G, Soler M. Antibody-dependent enhancement of dengue 2 virus in people of white descent in Cuba. Lancet. 1987;1:1028–9 . DOIPubMedGoogle Scholar
- Silva LK, Blanton RE, Parrado AR, Melo PS, Morato VG, Reis EA, Dengue hemorrhagic fever is associated with polymorphisms in JAK1. Eur J Hum Genet. 2010;18:1221–7 . DOIPubMedGoogle Scholar
- Gubler DJ, Sather GE, Kuno G, Cabral JR. Dengue 3 virus transmission in Africa. Am J Trop Med Hyg. 1986;35:1280–4 .PubMedGoogle Scholar
- Gubler DJ. The global pandemic of dengue/dengue haemorrhagic fever: current status and prospects for the future. Ann Acad Med Singapore. 1998;27:227–34 .PubMedGoogle Scholar
- Malik A, Earhart K, Mohareb E, Saad M, Saeed M, Ageep A, Dengue hemorrhagic fever outbreak in children in Port Sudan. J Infect Public Health. 2011;4:1–6 . DOIPubMedGoogle Scholar
- Petti CA, Polage CR, Quinn TC, Ronald AR, Sande MA. Laboratory medicine in Africa: a barrier to effective health care. Clin Infect Dis. 2006;42:377–82 . DOIPubMedGoogle Scholar
- Blacksell SD, Jarman RG, Gibbons RV, Tanganuchitcharnchai A, Mammen MP Jr, Nisalak A, Comparison of seven commercial antigen and antibody enzyme-linked immunosorbent assays for detection of acute dengue infection. Clin Vaccine Immunol. 2012;19:804–10 . DOIPubMedGoogle Scholar
- Guzman MG, Jaenisch T, Gaczkowski R, Ty Hang VT, Sekaran SD, Kroeger A, Multi-country evaluation of the sensitivity and specificity of two commercially-available NS1 ELISA assays for dengue diagnosis. PLoS Negl Trop Dis. 2010;4:e811 . DOIPubMedGoogle Scholar
- Hunsperger EA, Yoksan S, Buchy P, Nguyen VC, Sekaran SD, Enria DA, Evaluation of commercially available anti-dengue virus immunoglobulin M tests. Emerg Infect Dis. 2009;15:436–40 . DOIPubMedGoogle Scholar
- Santiago GA, Vergne E, Quiles Y, Cosme J, Vazquez J, Medina JF, Analytical and clinical performance of the CDC real time RT-PCR assay for detection and typing of dengue virus. PLoS Negl Trop Dis. 2013;7:e2311 . DOIPubMedGoogle Scholar
- Wang SM, Sekaran SD. Early diagnosis of dengue infection using a commercial Dengue Duo rapid test kit for the detection of NS1, IGM, and IGG. Am J Trop Med Hyg. 2010;83:690–5 . DOIPubMedGoogle Scholar
- Tricou V, Vu HT, Quynh NV, Nguyen CV, Tran HT, Farrar J, Comparison of two dengue NS1 rapid tests for sensitivity, specificity and relationship to viraemia and antibody responses. BMC Infect Dis. 2010;10:142 . DOIPubMedGoogle Scholar
- Blacksell SD, Jarman RG, Bailey MS, Tanganuchitcharnchai A, Jenjaroen K, Gibbons RV, Evaluation of six commercial point-of-care tests for diagnosis of acute dengue infections: the need for combining NS1 antigen and IgM/IgG antibody detection to achieve acceptable levels of accuracy. Clin Vaccine Immunol. 2011;18:2095–101 . DOIPubMedGoogle Scholar
- Sánchez-Vargas LA, Sanchez-Marce EE, Vivanco-Cid H. Evaluation of the SD BIOLINE dengue duo rapid test in the course of acute and convalescent dengue infections in a Mexican endemic region. Diagn Microbiol Infect Dis. 2014;78:368–72 . DOIPubMedGoogle Scholar
- World Health Organization. WHO report on global surveillance of epidemic-prone infectious diseases: dengue and dengue haemorrhagic fever, 2014 [cited 2014 Jul 21]. http://www.who.int/csr/resources/publications/dengue/CSR_ISR_2000_1/en/index3.html
- Sankoh O, Byass P. The INDEPTH Network: filling vital gaps in global epidemiology. Int J Epidemiol. 2012;41:579–88 . DOIPubMedGoogle Scholar
- Diallo M, Sall AA, Moncayo AC, Ba Y, Fernandez Z, Ortiz D, Potential role of sylvatic and domestic African mosquito species in dengue emergence. Am J Trop Med Hyg. 2005;73:445–9 .PubMedGoogle Scholar
- Brown JE, McBride CS, Johnson P, Ritchie S, Paupy C, Bossin H, Worldwide patterns of genetic differentiation imply multiple ‘domestications’ of Aedes aegypti, a major vector of human diseases. Proc Biol Sci. 2011;278:2446–54 . DOIPubMedGoogle Scholar
- Moore M, Sylla M, Goss L, Burugu MW, Sang R, Kamau LW, Dual African origins of global Aedes aegypti s.l. populations revealed by mitochondrial DNA. PLoS Negl Trop Dis. 2013;7:e2175 and. DOIPubMedGoogle Scholar
- Diallo M, Ba Y, Faye O, Soumare ML, Dia I, Sall AA. Vector competence of Aedes aegypti populations from Senegal for sylvatic and epidemic dengue 2 virus isolated in west Africa. Trans R Soc Trop Med Hyg. 2008;102:493–8 . DOIPubMedGoogle Scholar
- Paupy C, Brengues C, Ndiath O, Toty C, Herve JP, Simard F. Morphological and genetic variability within Aedes aegypti in Niakhar, Senegal. Infect Genet Evol. 2010;10:473–80 and. DOIPubMedGoogle Scholar
- Schoof HF. Mating, resting habits and dispersal of Aedes aegypti. Bull World Health Organ. 1967;36:600–1 .PubMedGoogle Scholar
- Lumsden WH. The activtiy cycle of domestic Aedes (Stegomyia) aegypti (L.) (Diptera: Culicidae) in Southern Province, Tanganyika. Bull Entomol Res. 1957;48:769–82. DOIGoogle Scholar
- Savage HM, Ezike VI, Nwankwo AC, Spiegel R, Miller BR. First record of breeding populations of Aedes albopictus in continental Africa: implications for arboviral transmission. J Am Mosq Control Assoc. 1992;8:101–3 .PubMedGoogle Scholar
- Kamgang B, Nchoutpouen E, Simard F, Paupy C. Notes on the blood-feeding behavior of Aedes albopictus (Diptera: Culicidae) in Cameroon. Parasit Vectors. 2012;5:57.PubMedGoogle Scholar
- Kamgang B, Happi JY, Boisier P, Njiokou F, Herve JP, Simard F, Geographic and ecological distribution of the dengue and chikungunya virus vectors Aedes aegypti and Aedes albopictus in three major Cameroonian towns. Med Vet Entomol. 2010;24:132–41 . DOIPubMedGoogle Scholar
- World Health Organization. Vector management and delivery of vector control services. Dengue guidelines for diagnosis, treatment, prevention and control. 3rd ed. Geneva: The Organization 2009.
- Lenhart A, Orelus N, Maskill R, Alexander N, Streit T, McCall PJ. Insecticide-treated bednets to control dengue vectors: preliminary evidence from a controlled trial in Haiti. Trop Med Int Health. 2008;13:56–67 . DOIPubMedGoogle Scholar
- Esu E, Lenhart A, Smith L, Horstick O. Effectiveness of peridomestic space spraying with insecticide on dengue transmission; systematic review. Trop Med Int Health. 2010;15:619–31 .PubMedGoogle Scholar
- Greif MJ, Dodoo FN, Jayaraman A. Urbanisation, poverty and sexual behaviour: the tale of five African cities. Urban Stud. 2011;48:947–57 . DOIPubMedGoogle Scholar
- United Nations. World urbanization prospects. The 2011 revision. New York: United Nations; 2012.
- Badurdeen S, Valladares DB, Farrar J, Gozzer E, Kroeger A, Kuswara N, Sharing experiences: towards an evidence based model of dengue surveillance and outbreak response in Latin America and Asia. BMC Public Health. 2013;13:607 . DOIPubMedGoogle Scholar
- Zorlu G, Fleck F. Dengue vaccine roll-out: getting ahead of the game. Bull World Health Organ. 2011;89:476–7 . DOIPubMedGoogle Scholar
Figure
Suggested citation for this article: Jaenisch T, Junghanss T, Wills B, Brady OJ, Eckerle I, Farlow A, et al. Dengue expansion in Africa—not recognized or not happening? Emerg Infect Dis [Internet]. 2014 Oct [date cited]. http://dx.doi.org/10.3201/eid2010.140487
1Members of the Dengue in Africa Study Group are listed at the end of this article.
Table of Contents – Volume 20, Number 10—October 2014
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Thomas Jaenisch, Department of Infectious Diseases, Section Clinical Tropical Medicine, Heidelberg University Hospital, INF 324, Heidelberg 69126, Germany
Top