Volume 20, Number 8—August 2014
Dispatch
Severe Murine Typhus with Pulmonary System Involvement
Cite This Article
Citation for Media
Abstract
We encountered a case of severe murine typhus complicated by acute respiratory distress syndrome. To determine worldwide prevalence of such cases, we reviewed the literature and found that respiratory symptoms occur in ≈30% of murine typhus patients. In disease-endemic areas, murine typhus should be considered for patients with respiratory symptoms and fever.
Murine typhus (endemic typhus) is a febrile illness caused by fleaborne Rickettsia typhi; it occurs mainly in environments where rats and humans live in close proximity. Murine typhus is found worldwide, but most reported cases originate from Southeast Asia, the Mediterranean region, and the United States. Among travelers, murine typhus is most frequently associated with travel to Southeast Asia (1). Recently, 2 cases of severe murine typhus with pulmonary manifestations have been reported (2,3). Near the same time, the Academic Medical Center (Amsterdam, the Netherlands) admitted a patient with severe murine typhus and respiratory failure. On the basis of these 3 cases, we hypothesized that pulmonary system involvement of murine typhus might be more common than previously assumed. We conducted this study because data on prevalence of pulmonary involvement in murine typhus are rarely reported. We therefore describe a clinical case and summarize the published literature on the pulmonary aspects of murine typhus.
In February 2012, a previously healthy 40-year-old man visited the Academic Medical Center outpatient department, reporting fever, headache, sweating, and nausea. The signs and symptoms had started 1 day earlier, on the day of his return from a 1-month holiday in Borneo. He reported frequent insect bites and exposure to fresh water. He had taken malaria chemoprophylaxis as recommended, and his vaccinations were up to date. Physical examination indicated that he was afebrile, was hemodynamically stable, and had a discrete macular rash on the trunk but no eschar. Laboratory results showed a hemoglobin concentration (16.8 g/dL) within reference range, a leukocyte count of 4,700 cells/mm3 with lymphopenia (1,090 cells/mm3), and thrombocytopenia (116,000 cells/mm3). C-reactive protein (42 mg/L) and serum creatinine (1.32 mg/dL) concentrations were moderately elevated. A thick smear showed no plasmodia, and a dengue antigen test result was negative. By the next day, the patient’s condition had deteriorated; he was experiencing chills, his temperature was 39°C, and the rash had become more pronounced. He was admitted to the hospital and given doxycycline (200 mg twice a day) for suspected rickettsiosis or leptospirosis. After admission, his condition deteriorated further; increasing dyspnea progressed to respiratory failure, necessitating intubation and admission to the intensive care unit on the second day after admission.
Figure
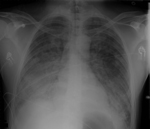
Figure. Chest radiograph of 40-year-old man with acute respiratory distress syndrome as a complication of murine typhus.
Chest radiographs revealed bilateral interstitial abnormalities (Figure). His condition fit a diagnosis of acute respiratory distress syndrome (ARDS). Empirical treatment was expanded to include broad-spectrum antimicrobial drugs and oseltamivir.
On the fourth day of intubation, the patient’s condition improved; he was extubated 1 day later. Cultured blood, urine, and bronchial fluid remained sterile, and test results for Leptospira, Legionella, influenza virus, and HIV were negative. All antimicrobial drugs except doxycycline were discontinued; doxycycline was continued for a total of 14 days.
Serum collected 1 day after admission showed weakly positive IgG against R. typhi; after 7 days, the immunofluorescent antibody titer had increased 4-fold (from 1:64 to >1:256). The patient recovered completely and was doing well at his last follow-up visit.
To determine prevalence of such cases, we conducted a search of published studies mentioning pulmonary manifestations of murine typhus (details in the Technical Appendix). From 779 records, we selected 22 cohort studies and 18 case studies that, according to title and abstract, were relevant to our research question. We differentiated between studies with individual patient data (case reports and case series) and studies without individual patient data (cohort studies). For each study, we recorded year of publication, study design, and country of infection. We also recorded the presence of pulmonary involvement, defined as cough and any mention of an abnormal finding on chest radiograph, without further distinction.
An overview of study characteristics detailing prevalence of cough and chest radiograph abnormalities is provided in the Technical Appendix Table 1. Two studies were prospective population-based studies of the causative agent of fever of unknown origin. The remaining 20 studies were all Rickettsia spp. specific; in 17 of these studies, patients had been recruited retrospectively from hospital databases or chart reviews.
The 22 study reports that contained data on the presence or absence of cough together accounted for 1,060 patients with murine typhus. The prevalence of cough among these patients ranged from 0 to 66%. Mean prevalence (all patients from all studies combined) of cough was 30.1% (95% CI 23.3–36.9).
Data on presence or absence of radiographic abnormalities were mentioned in 9 study reports (4–12). Taken together, these studies evaluated 621 patients and 104 chest radiographs showing abnormalities, leading to a prevalence rate of chest radiograph abnormalities of 16.7% (95% CI 8.21–25.5). The cohort studies reported 2 cases of ARDS, 1 with a fatal outcome. The Table shows the full-text descriptions of chest radiograph abnormalities.
Pulmonary manifestations were also documented by the case studies. Among these studies, 2 patients had ARDS, 7 had bilateral pulmonary infiltrates, 5 had unilateral pulmonary infiltrates, 1 had pulmonary embolism, and 1 had respiratory failure (no chest radiograph was reported) (Technical Appendix Table 2). We also found that cough occurred more commonly among patients in studies conducted in Asia (99 [38.2%] of 259 patients) than among those in studies conducted in the Mediterranean region (118 [25.8%] of 457) and North America (56 [23.3%] of 240).
In the literature, we found 7 reported cases of respiratory distress associated with murine typhus (including the case reported here), 2 of which described respiratory distress not classified as ARDS (2,13). Of these 7 case-patients with ARDS/respiratory distress, 5 (71%) patients were from Asia (2,3,11,13), 1 was from the Mediterranean region (4), and 1 was from the United States (14).
Cough and chest radiograph abnormalities were frequent manifestations of murine typhus. For cough associated with murine typhus, we found a prevalence rate of ≈30%. The prevalence of chest radiograph abnormalities was more difficult to ascertain because this result was less often reported and more influenced by bias. The pulmonary aspects of R. typhi infection are probably the result of damaged pulmonary microcirculation, leading to pulmonary edema.
Severe pulmonary manifestations of murine typhus are thought to be rare. The case reported here is unusual in that the symptoms progressed rapidly and the response to doxycycline was relatively slow. It is worth noting that we found no more than 2 reported cases of fatal murine typhus associated with pulmonary system disease; both were the result of severe disease complicated by ARDS.
In addition, we noted possible geographic variation in pulmonary manifestations. Most cases of severe murine typhus with pulmonary manifestations originated in Asia, and cough was more frequently a symptom among patients in Asia.
The primary strength of our study is the extensive literature search, which covered studies from different parts of the world and included cohort studies and case series. The main limitation of this study is the retrospective nature of the data collection for most studies, which is prone to bias and renders meaningful statistical analysis of results impossible. Therefore, prospective studies evaluating pulmonary manifestations of murine typhus and possible geographic variation are needed.
Although murine typhus usually follows a benign course, severe disease with pulmonary manifestations, including ARDS, can occur, as described for the patient reported here. We suggest that murine typhus should be included in the differential diagnosis for any patient who has a fever and respiratory signs and who has been in a typhus-endemic area within the incubation period.
Mr van der Vaart is a sixth-year medical student at the Academic Medical Center of the University of Amsterdam and is currently enrolled in his clinical rotations. His main research focus is infectious diseases.
References
- Jensenius M, Han PV, Schlagenhauf P, Schwartz E, Parola P, Castelli F, Acute and potentially life-threatening tropical diseases in western travelers—a GeoSentinel multicenter study, 1996–2011. Am J Trop Med Hyg. 2013;88:397–404 . DOIPubMedGoogle Scholar
- Stockdale AJ, Weekes MP, Kiely B, Lever AM. Case report: severe typhus group rickettsiosis complicated by pulmonary edema in a returning traveler from Indonesia. Am J Trop Med Hyg. 2011;85:1121–3. DOIPubMedGoogle Scholar
- Sakamoto N, Nakamura-Uchiyama F, Kobayashi K, Takasaki T, Ogasawara Y, Ando S, Severe murine typhus with shock and acute respiratory failure in a Japanese traveler after returning from Thailand. J Travel Med. 2013;20:50–3. DOIPubMedGoogle Scholar
- Bernabeu-Wittel M, Pachon J, Alarcon A, Lopez-Cortes LF, Viciana P, Jimenez-Mejias ME, Murine typhus as a common cause of fever of intermediate duration: a 17-year study in the south of Spain. Arch Intern Med. 1999;159:872–6. DOIPubMedGoogle Scholar
- Whiteford SF, Taylor JP, Dumler JS. Clinical, laboratory, and epidemiologic features of murine typhus in 97 Texas children. Arch Pediatr Adolesc Med. 2001;155:396–400. DOIPubMedGoogle Scholar
- Gikas A, Doukakis S, Pediaditis J, Kastanakis S, Manios A, Tselentis Y. Comparison of the effectiveness of five different antibiotic regimens on infection with Rickettsia typhi: therapeutic data from 87 cases. Am J Trop Med Hyg. 2004;70:576–9 .PubMedGoogle Scholar
- Zimmerman MD, Murdoch DR, Rozmajzl PJ, Basnyat B, Woods CW, Richards AL, Murine typhus and febrile illness, Nepal. Emerg Infect Dis. 2008;14:1656–9. DOIPubMedGoogle Scholar
- Gikas A, Kokkini S, Tsioutis C, Athenessopoulos D, Balomenaki E, Blasak S, Murine typhus in children: clinical and laboratory features from 41 cases in Crete, Greece. Clin Microbiol Infect. 2009;15(Suppl 2):211–2. DOIGoogle Scholar
- Suputtamongkol Y, Suttinont C, Niwatayakul K, Hoontrakul S, Limpaiboon R, Chierakul W, Epidemiology and clinical aspects of rickettsioses in Thailand. Ann N Y Acad Sci. 2009;1166:172–9 and. DOIPubMedGoogle Scholar
- Chaliotis G, Kritsotakis EI, Psaroulaki A, Tselentis Y, Gikas A. Murine typhus in central Greece: epidemiological, clinical, laboratory, and therapeutic-response features of 90 cases. Int J Infect Dis. 2012;16:e591-6. DOIGoogle Scholar
- Chang K, Chen YH, Lee NY, Lee HC, Lin CY, Tsai JJ, Murine typhus in southern Taiwan during 1992–2009. Am J Trop Med Hyg. 2012;87:141–7. DOIPubMedGoogle Scholar
- Znazen A, Hammami B, Mustapha AB, Chaari S, Lahiani D, Maaloul I, Murine typhus in Tunisia: a neglected cause of fever as a single symptom. Med Mal Infect. 2013;43:226–9. DOIPubMedGoogle Scholar
- Tan L, Beersma TM, van Beek Y, van Genderen PJ. Two travellers suffering from typhus [in Dutch]. Ned Tijdschr Geneeskd. 2011;155:A3845 .PubMedGoogle Scholar
- Walker DH, Parks FM, Betz TG, Taylor JP, Muehlberger JW. Histopathology and immunohistologic demonstration of the distribution of Rickettsia typhi in fatal murine typhus. Am J Clin Pathol. 1989;91:720–4 .PubMedGoogle Scholar
Figure
Table
Cite This ArticleTable of Contents – Volume 20, Number 8—August 2014
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Address for correspondence: Abraham Goorhuis, Center for Tropical and Travel Medicine, Division of Infectious Diseases, Department of Internal Medicine, Academic Medical Center, University of Amsterdam, Meibergdreef 9, Room F4-217, 1105 AZ Amsterdam, the Netherlands
Top