Volume 20, Number 8—August 2014
Dispatch
Co-circulation of Dengue and Chikungunya Viruses, Al Hudaydah, Yemen, 2012
Cite This Article
Citation for Media
Abstract
We investigated 400 cases of dengue-like illness in persons hospitalized during an outbreak in Al Hudaydah, Yemen, in 2012. Overall, 116 dengue and 49 chikungunya cases were diagnosed. Dengue virus type 2 was the predominant serotype. The co-circulation of these viruses indicates that mosquitoborne infections represent a public health threat in Yemen.
Vectorborne infections are not uncommon in the Middle East (1). In particular, recurrent outbreaks of dengue fever have been reported on the Arabian Peninsula since 1990 (2). In Yemen, dengue virus (DENV) infections have reemerged with higher frequency during the last decade (3); in 2010, during a dengue outbreak that occurred in the southern governorate of Hadramout (4), cases of dengue hemorrhagic fever were identified (5). In 2010–2011, another mosquitoborne virus, the chikungunya virus (CHIKV), was detected in febrile patients in Al Hudaydah, Yemen (6). To evaluate to what extent these arboviruses are involved in dengue-like illness outbreaks in Yemen, we conducted a study in Al Hudaydah.
Figure 1

Figure 1. Location of Al Hudaydah, Yemen, where the co-circulation of dengue virus, chikungunya virus, and other dengue-like viruses was studied in 2012Other important towns, Sanaa, Aden, and Al Mukalla (the capital of...
The study site was represented by 5 hospital centers (Renal Center, Maritime College, Al Rasheed, Al-Thawra, Al Salakhana) located in Al Hudaydah (Figure 1). Patients hospitalized during 2012 were recruited for the study if they had fever (>37.5°C) and at >2 of the following signs or symptoms at the time of admission: headache, joint pain, muscle pain, skin rash. Serum samples were collected within 4 days from the date of hospital admission and stored and shipped at −20°C.
We used the Maxwell 16 Viral Total Nucleic Acid Purification Kit with the Maxwell 16 instrument (Promega, Madison, WI, USA) according to the manufacturer's instructions to extract nucleic acids from the serum samples. We then analyzed the nucleic acids by using DENV- and CHIKV-specific PCR sequences, as previously described for DENV and adapted for CHIKV (7,8). To further confirm the results, we amplified and then sequenced NS1 and E1 genes from DENV- and/or CHIKV-positive serum samples; the sequences were deposited in GenBank (accession nos. KJ742803–19).
We used the NovaLisa Dengue IgM- and IgG-ELISAs and the NovaLisa Chikungunya IgM- and IgG-capture ELISAs (NovaTec lmmundiagnostica GmbH, Dietzenbach, Germany) according to the manufacturer’s instructions to analyze serum samples for IgM and IgG. Study participants with IgM ELISA– and/or PCR-positive results were defined as recently or acutely infected with DENV or CHIKV.
Overall, 400 persons were enrolled in the study. The median age was 30 years (range 1–60). The median interval between fever onset and sample collection was 4 days (range 2–9).
Of the 400 study participants, 116 (29%) were IgM or PCR positive for DENV RNA. Of those 116 persons, 61 (53%) had IgM, 44 (38%) were positive by PCR, and 11 (9%) had IgM- and PCR-positive results. Of the 55 PCR-positive samples, 41 were DENV-2 and 2 DENV-1. The remaining 12 samples were not typed because the virus titer was low, and it was not possible to achieve a positive signal by using a DENV serotype–specific PCR. Of the 400 study participants, 290 (72.5%) had IgG against DENV. Their distribution by diagnostic category is shown in Table 1.
Of the 400 participants, 49 (12%) were IgM and/or PCR positive for CHIKV RNA: 38 (77%) were IgM positive, 10 (20%) were PCR positive, and 1 was positive by both methods. Of the 351 patients with negative IgM/PCR results, 33 (9.4%) had IgG against CHIKV.
No samples were PCR positive for both viruses. However, 13 samples had IgM against both viruses, and 1 had positive results for DENV by PCR and CHIKV IgM by ELISA.
Figure 2
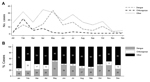
Figure 2. Trends for cases of dengue virus, chikungunya virus, and other dengue-like viruses, Al Hudaydah, Yemen, 2012A) Number of cases by monthB) Monthly percentages of cases by virus type.
The monthly distribution and the proportion of DENV- and CHIKV-positive cases are shown in Figure 2. Peaks were observed during February, when the highest number of chikungunya cases was observed, and especially May, when the highest number of dengue fever cases was observed. A low number of cases were reported in November and December.
Study participants with CHIKV infection (mean age 30.67 years, + SD 14.17 years) were slightly younger than with DENV infection (mean age 27.53 years, + standard deviation 17.34 years), but the median age (30 years) and range (1–60 years) were the same for the 2 groups. The distribution of signs and symptoms for recent/acute cases of dengue and chikungunya are shown in Table 2. The most common signs symptoms for both infections were joint pain (98%), myalgia (95% and 94%, respectively), and headache (94% and 88%, respectively). Persons with chikungunya were more likely than those with dengue to report vomiting (41% vs. 25%). No other major difference in the frequency of specific signs or symptoms was found.
Our data provide evidence of co-circulation of CHIKV and 2 DENV serotypes in the governorate of Al Hudaydah. DENV-2 was the predominant serotype in our study population. Whether this serotype was newly introduced into Yemen in 2012 is unknown. In 2011 in the same area, a small study was conducted with 47 patients with dengue-like illness, and only 3 were PCR positive for DENV: 2 for DENV-1 and 1 for DENV-3 (data not shown). In 2010 in Al Mukalla, the capital of the district of Hadramout, DENV-3 was also detected in patients with dengue fever and dengue hemorrhagic fever (5,9).
The high prevalence (>70%) of DENV IgG in our study population suggests past exposure to DENV. Relatively high rates of IgG were also found during the outbreak that occurred in 2011 in Hadramout, where 28% of DENV IgM–positive and 43% of DENV IgM–negative patients with dengue-like illness were positive for DENV IgG (4). The identification of dengue hemorrhagic fever cases caused by DENV-3 in Al Mukalla is also suggestive of exposure to different DENV serotypes (5). The hypothesis of continued reintroduction of different DENV serotypes in Yemen dates back to 1983, when a secondary heterotypic DENV infection was suspected in a man who had traveled from Dalah (160 miles from Aden), an area endemic for DENV. The traveler had dengue hemorrhagic fever and high antibody titers against all 4 DENV serotypes (10). It is well known that travels to and from DENV-endemic areas are common, and imported cases from eastern Africa (Zanzibar) were reported in Yemen as early as the nineteenth century (11,12). Circulation of different DENV serotypes has also been reported in Saudi Arabia: DENV-3 emerged as the predominant serotype after 1997, and DENV-2 and DENV-1 serotypes had been associated with earlier outbreaks (13).
We identified a rather large number of cases of recent or acute CHIKV infection. This finding is consistent with a previous estimate of 1,542 cases during October 2010–January 2011 (6) and with the detection of CHIKV RNA in Aedes aegypti mosquitoes, the dominant type of mosquito in entomologic investigations conducted in Al Hudaydah (14).
The circulation of mosquitoborne viruses in a dry area like Yemen is not surprising. Water scarcity and lack of infrastructure in periurban areas require regular storage of water for household and potable use, and water containers favor A. aegypti mosquito reproduction. Moreover, increasing migration and urbanization may favor the introduction and spread of these infections (15).
Our study did have some limitations. First, the study was hospital based. Thus, the findings may not be representative of the whole epidemic in the community. Second, some misclassification of the cases caused by the sensitivity and specificity of the tests or to a time lag between symptom onset and sample collection (i.e., PCR- or IgM-negative results caused by testing intervals that were too long or too short, respectively) cannot be ruled out. Last, the prevalence of IgG against DENV might have been overestimated because of possible cross-reactivity with other flavivirus infections.
In conclusion, CHIKV and various DENV serotypes co-circulate in Yemen’s port city of Al Hudaydah. The detection of CHIKV and DENV IgG–positive persons suggests that these viruses are either endemic or continuously reintroduced to the area. Mosquito control activities are needed to reduce the effect of arbovirus infections on public health.
Dr Rezza is an infectious diseases epidemiologist and currently Head of the Department of Infectious, Parasitic and Immunomediated Diseases of the Italian National Institute of Health. He is an expert in the field of emerging infections, with particular regard to viral infections, such as HIV, human herpesvirus type 8, pandemic influenza, and arboviruses.
Acknowledgment
We thank Anna Carinci for editorial assistance in the revision of the manuscript.
References
- Hotez PJ, Savioli L, Fenwick A. Neglected tropical diseases of the Middle East and North Africa: review of their prevalence, distribution, and opportunities for control. PLoS Negl Trop Dis. 2012;6:e1475 . DOIPubMedGoogle Scholar
- Ooi EE, Gubler DJ. Dengue and dengue hemorrhagic fever. In: Guerrant RL, Walker DH, Weller PF, editors. Tropical infectious diseases: principles, pathogens and practice. 3rd ed. Toronto: Saunders Elsevier; 2011.
- World Health Organization and the Special Programme for Research and Training in Tropical Diseases. Dengue: guidelines for diagnosis, treatment, prevention and control: new edition. Geneva: The Organization; 2009.
- Bin Ghouth AS, Amarasingh A, Letson W. Dengue outbreak in Hadramout, Yemen, 2010: an epidemiological perspective. Am J Trop Med Hyg. 2012;86:1072–6 . DOIPubMedGoogle Scholar
- Madani TA, Abuelzein ETM, Al-Bar HM, Azhar EI, Kao M, Alshoeb HO, Outbreak of viral hemorrhagic fever caused by dengue virus type 3 in Al-Mukalla, Yemen. BMC lnfect Dis. 2013;13:136.
- EpiSouth Network. EpiSouth Weekly Epi Bulletin (e-WEB), no. 155. Report of new health events occurring outside the EpiSouth area (not occurring in one or several EpiSouth countries): chikungunya, Yemen; 2011 Mar 10 [cited 2013 Aug 21]. http://www.episouthnetwork.org/content/episouth-weekly-epi-bulletin-e-web
- Leparc-Goffart I, Baragatti M, Temmam S, Tuiskunen A, Moureau G, Charrel R, Development and validation of real-time one-step reverse transcription-PCR for the detection and typing of dengue viruses. J Clin Virol. 2009;45:61–6 . DOIPubMedGoogle Scholar
- Pastorino B, Bessaud M, Grandadam M, Murri S, Tolou HJ, Peyrefitte CN. Development of a TaqMan RT-PCR assay without RNA extraction step for the detection and quantification of African Chikungunya viruses. J Virol Methods. 2005;124:65–71 . DOIPubMedGoogle Scholar
- Ravanini P, Huhtamo E, Hasu E, Rosa F, Costantino S, Crobu MG, lmported dengue virus serotype 3, Yemen to Italy, 2010. Emerg Infect Dis. 2011;17:929–31 . DOIPubMedGoogle Scholar
- Jimenez-Lucho VE, Fisher EJ, Saravolatz LD. Dengue with hemorrhagic manifestations: an imported case from the Middle East. Am J Trop Med Hyg. 1984;33:650–3 .PubMedGoogle Scholar
- Christie CJ. Dengue. BMJ. 1872;2:244.
- Radcliffe JN. Dengue. BMJ. 1877;1:25–6.
- Shibl A, Senok A, Memish Z. Infectious diseases in the Arabian Peninsula and Egypt. Clin Microbiol Infect. 2012;18:1068–80 . DOIPubMedGoogle Scholar
- Zayed A, Awash AA, Esmal MA, Al-Mohamadi HA, Al-Salwai M, Al-Jasari A, Detection of Chikungunya virus in Aedes Aegypti during the 2011 outbreak in Al Hodayda, Yemen. Acta Trop. 2012;123:62–6 . DOIPubMedGoogle Scholar
- Amarasinghe A, Letson GW. Dengue in the Middle East: a neglected, emerging disease of importance. Trans R Soc Trop Med Hyg. 2012;106:1–2 . DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 20, Number 8—August 2014
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Giovanni Rezza, Department of Infectious, Parasitic and Immunomediated Diseases, Istituto Superiore di Sanità, Viale Regina Elena, 299, 00161 Roma, Italy
Top