Volume 24, Number 4—April 2018
Research
Influence of Population Immunosuppression and Past Vaccination on Smallpox Reemergence
C. Raina MacIntyre, Valentina Costantino , Xin Chen, Eva Segelov, Abrar Ahmad Chughtai, Anthony Kelleher, Mohana Kunasekaran, and John Michael Lane
, Xin Chen, Eva Segelov, Abrar Ahmad Chughtai, Anthony Kelleher, Mohana Kunasekaran, and John Michael Lane
Figure 4
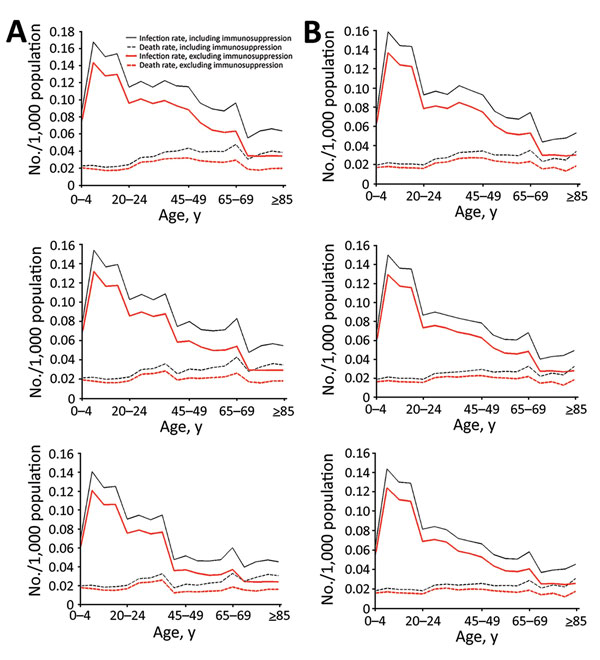
Figure 4. Smallpox infection and death rates with different levels of residual vaccine immunity including and excluding immunosuppression in model of smallpox transmission, by age group, New York, NY, USA, and Sydney, Australia. Characteristics (e.g., size, age, immunosuppression rates) of populations from 2015 were used. A) New York 50 days after start of smallpox outbreak with no (top), base case (middle), and high (bottom) residual vaccine immunity. B) Sydney 50 days after start of smallpox outbreak with no (top), base case (middle), and high (bottom) residual vaccine immunity.
Page created: March 20, 2018
Page updated: March 20, 2018
Page reviewed: March 20, 2018
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.