Volume 24, Number 7—July 2018
Perspective
Effects of Sexual Network Connectivity and Antimicrobial Drug Use on Antimicrobial Resistance in Neisseria gonorrhoeae
Figure 2
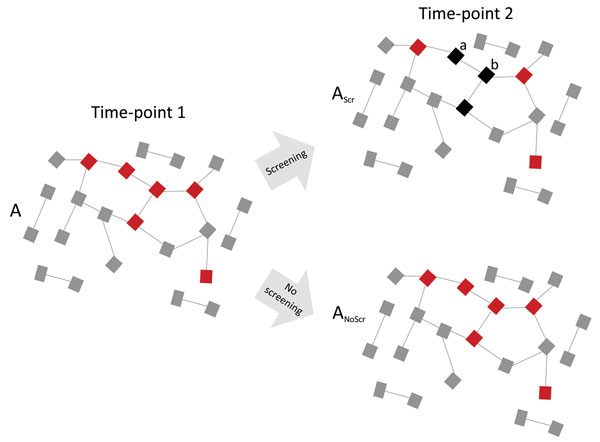
Figure 2. Diagram showing how high network connectivity combined with excess antimicrobial drug exposure from Neisseria gonorrhoeae preexposure prophylaxis could produce antimicrobial resistance (AMR). A dense sexual network translates into a high equilibrium prevalence of N. gonorrhoeae (red squares) at time point 1. Active N. gonorrhoeae screening of 50% of this population every 3 months results in 50% lower N. gonorrhoeae prevalence at time-point 2 (3 months later) but at the expense of an altered resistome (AScr; black squares represent 3 patients with N. gonorrhoeae cleared by screening and treatment). The unchanged underlying network connectivity means that the prevalence of antimicrobial-sensitive N. gonorrhoeae is now 50% of its equilibrium prevalence, but if it acquired AMR it could return to its equilibrium prevalence. Furthermore, recently cured patients (a and b) are at high risk for reinfection from their partners at a time when their resistomes are enriched with resistance genes. Early reinfecting N. gonorrhoeae can acquire AMR by taking up these resistance genes by transformation. The screening program has thus both placed a selection pressure for the emergence of AMR and provided the resistance genes needed for AMR. In the absence of screening and excess antimicrobial drug use (ANoScr), N. gonorrhoeae prevalence would not decline, but there would be no pressure to select for antimicrobial resistance. Gray squares indicate uninfected persons; lines represent sexual relationships.