Classification of Trauma-Associated Invasive Fungal Infections to Support Wound Treatment Decisions
Anuradha Ganesan

, Faraz Shaikh, William Bradley, Dana M. Blyth, Denise Bennett, Joseph L. Petfield, M. Leigh Carson, Justin M. Wells, David R. Tribble, and Infectious Disease Clinical Research Program Trauma Infectious Disease Outcomes Study Group
Author affiliations: The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., Bethesda, Maryland, USA (A. Ganesan, F. Shaikh, W. Bradley, D. Bennett, M.L. Carson); Uniformed Services University of the Health Sciences, Bethesda (A. Ganesan, F. Shaikh, W. Bradley, D. Bennett, M.L. Carson, D.R. Tribble); Walter Reed National Military Medical Center, Bethesda (A. Ganesan, J.M. Wells); Brooke Army Medical Center, San Antonio, Texas, USA (W. Bradley, D.M. Blyth); Landstuhl Regional Medical Center, Landstuhl, Germany (J.L. Petfield)
Main Article
Figure 1
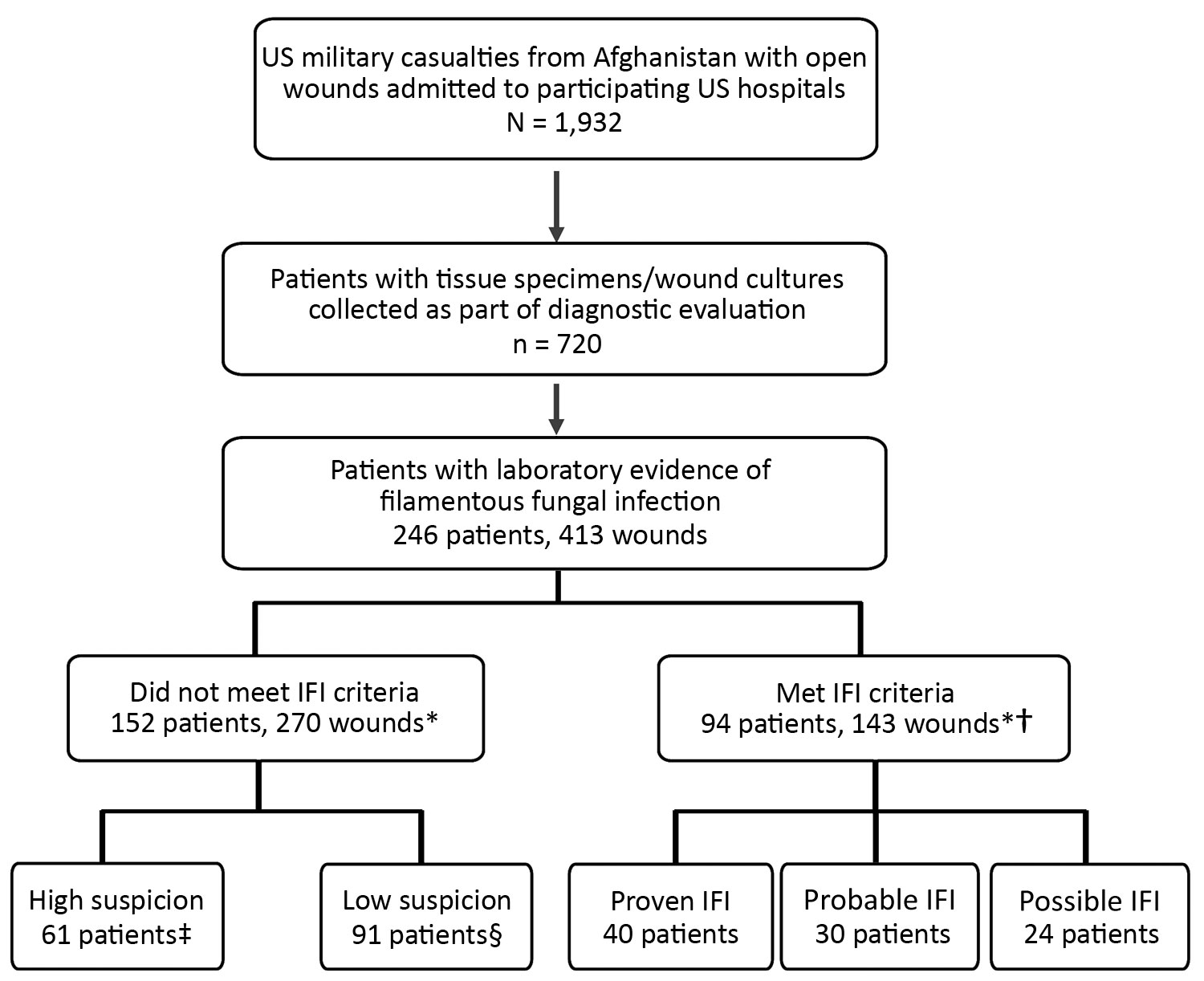
Figure 1. Combat casualties with laboratory evidence of fungal infection in study of US military patients who had laboratory evidence of fungal infection after battlefield trauma in Afghanistan, June 1, 2009–December 31, 2014. *Total of 143 IFI wounds, 120 high-suspicion wounds, and 150 low-suspicion wounds. For the person-level analysis, patients with multiple wounds were included in the IFI group even if 1 of their wounds met criteria other than for an IFI; similarly, patients with both low-suspicion and high-suspicion wounds were included in the high-suspicion group. †94 patients had 143 wounds that met criteria for an IFI; these same patients had 31 wounds that met criteria for high-suspicion wounds and 16 wounds that met criteria for low-suspicion wounds. ‡61 patients had 89 wounds that met criteria for high-suspicion wounds and 14 wounds that met criteria for low-suspicion wounds. §91 patients had 120 wounds classified as low-suspicion wounds. IFI, invasive fungal infection.
Main Article
Page created: August 20, 2019
Page updated: August 20, 2019
Page reviewed: August 20, 2019
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.