Volume 29, Number 4—April 2023
Research Letter
Orf Nodule with Erythema Multiforme during a Monkeypox Outbreak, France, 2022
Cite This Article
Citation for Media
Abstract
A 26-year-old patient in France who worked as a butcher sought care initially for erythema multiforme. Clinical examination revealed a nodule with a crusty center, which upon investigation appeared to be an orf nodule. Diagnosis was confirmed by PCR. The patient was not isolated and had a favorable outcome after basic wound care.
Orf nodule is a rare viral zoonosis attributable to an infection caused by a parapoxvirus (1). It is transmitted to humans by contact with sheep or goats that are affected by contagious ecthyma. The term orf is used to designate contagious ovine pustular dermatitis. In infected sheep and goats, infection most often results in perioral and perinasal ulcerations but occasionally also in a generalized pustular rash.
The most at risk for exposure are persons working in the meat sector, such as farmers or butchers (1). Farmers and those who maintain animal herds are often familiar with the condition and do not seek medical attention. Clinical visits for orf may therefore be more common among nonfarmers. Incidence often peaks at the time of religious festivals, when sheep are traditionally sacrificed, and the incubation time is approximately 1 week (2). The diagnosis is basically clinical and can be confirmed with PCR (3). Orf nodules may resemble mpox lesions, but unlike mpox, orf is not transmitted from human to human. Routine precautions in clinical settings are sufficient, and patients are not recommended to isolate.
In August 2022, a 26-year-old man with no notable medical history visited an emergency department for disseminated skin lesions predominantly in acral areas. The patient lives with his wife and children in Franche-Comté, France, and works as a butcher. He denied extraconjugal sex, including sex with men, and using illicit drugs, and he had not traveled recently. Neither fever nor contagion was reported. His attending physician prescribed local antibiotics (fucidin acid) and oral antibiotic drugs (amoxicillin/clavulanate), with no effect.
Figure
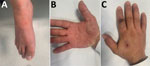
Figure. Orf virus infection in a 26-year-old man after contact with slaughtered sheep and goats, France, 2022. A, B) Target lesion characteristic of erythema multiforme predominant on the foot (A) and...
Clinical examination revealed symmetric maculopapular lesions predominantly on the palms and foot, with purplish center and pinkish halo (target shaped lesions), typical of erythema multiforme (Figure, panel A, B). Results of respiratory and neurologic examinations were unremarkable. A nodule with a necrotic pustule center was surrounded by a grayish-white edematous crown on the left index finger, suggesting a lesion of orf nodule more than a monkeypox infection (Figure, panel C). This lesion appeared 72 hours before the disseminated cocoon lesions, according to the patient.
Laboratory findings showed white cell count of 9.2 G/L (reference range 4–10 G/L) but lymphopenia of 880/mm3 (reference range 1,500–4,000/mm3). C-reactive protein was moderately high at 10 mg/L (reference range <5 mg/L); liver function was normal. Results of PCR for herpes simplex viruses 1 and 2 on skin biopsy were negative, as were serologic tests for Mycoplasma pneumoniae, HIV, and hepatitis B and C viruses. Because of the ongoing mpox outbreak, PCR for monkeypox virus was, performed after simple swabbing on the pustule, but results were negative.
Parapoxvirus PCR was performed by swab of nodule (on the left index finger) (Figure, panel C). The sample was sent to the National Reference Center for Orthopoxvirus Expert Laboratory (3). The laboratory used 2 real-time PCRs to confirm the diagnosis of orf nodule. The first assay detected parapoxvirus on the basis of the B2L and J6R genes; the second assay detected orf virus on the basis of the V22R and J6R genes. The patient was discharged with basic wound care, discontinuation of antibiotics, and a follow-up appointment 1 week later. At follow-up, erythema multiforme had disappeared and the nodule clinical regressed.
In typical forms, orf nodule is a skin lesion, unique to the area of inoculation, in particular the right fingers and forearm. A macular lesion appears and rapidly becomes papulovesicular, then nodular, surrounded by an inflammatory halo. Other forms include botriomycoid, angiomatous, or keratoacanthoma-like. The lesion generally heals without complication with antiseptic treatment in 4–6 weeks but in rare cases, erythema multiforme develops (2,4,5).
How orf virus induces erythema multiforme is not clearly understood. Other viral infections like herpes simplex viruses can also trigger hypersensitivity reaction because of release of T cells triggered by ether viral mimicry of host proteins or release of viral proteins from cells containing viral DNA fragments (1).
In this case, the patient experienced inaugural erythema multiforme and secondarily a suspected lesion of orf nodule in a period when monkeypox virus infection was endemic (i.e., >4,000 orthopoxvirus infections have been reported in France since May 2022) (6). Lesions of monkeypox and orf can be similar, but the manifestations are sufficiently distinctive (7,8). In this case, orf virus infection was suspected because of the patient’s occupational exposure and clinical compatible skin lesions (e.g., single pustular lesion and erythema multiforme aspect on the rest of the body and the absence of systemic symptoms) (9); infection was diagnosed with positive parapoxvirus PCR test (3). However, an unusual recent case in Portugal involved monkeypox infection after a needle stick injury (10). The patient had a solitary pustular lesion of the finger, similar to our patient, but that lesion was painful, and the clinical picture was completed with the appearance of diffuse vesicles and systemic symptoms.
This case highlights the importance of collecting a careful history at the time of patient care, including collection of exposures to possible zoonoses. Those measures are warranted to avoid unnecessary isolation and treatment and to enable appropriate infection control measures.
Dr. Zayet is a specialist in the Infectious Diseases Department of Nord Franche-Comte Hospital, Trevenans, France. His primary research interests focus on hepatitis and tuberculosis, especially in HIV-infected patients and COVID-19 patients.
Acknowledgments
C.C. and S.Z. were the major contributors in writing the manuscript and performing the literature review. A.S.D. provided the pictures and the legend. A.F.R. and O.F. conducted the microbiologic study. T.K. revised the manuscript. Both lead authors have read and agreed to the published version of the manuscript. The data presented in this case study are available on request from the corresponding author.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors declare no conflicts of interest.
References
- Haig DM, McInnes C, Deane D, Reid H, Mercer A. The immune and inflammatory response to orf virus. Comp Immunol Microbiol Infect Dis. 1997;20:197–204. DOIPubMedGoogle Scholar
- Ghislain PD, Dinet Y, Delescluse J. [Orf in urban surroundings and religious practices: a study over a 3-year period] [in French]. Ann Dermatol Venereol. 2001;128:889–92.PubMedGoogle Scholar
- Delaune D, Iseni F, Ferrier-Rembert A, Peyrefitte CN, Ferraris O. The French Armed Forces Virology Unit: a chronological record of ongoing research on orthopoxvirus. Viruses. 2017;10:3. DOIPubMedGoogle Scholar
- Joseph RH, Haddad FA, Matthews AL, Maroufi A, Monroe B, Reynolds M. Erythema multiforme after orf virus infection: a report of two cases and literature review. Epidemiol Infect. 2015;143:385–90. DOIPubMedGoogle Scholar
- Maman M, Medhioub Y. [A case of Orf disease complicated by erythema multiforme] [in French]. Arch Pediatr. 2017;24:1241–3. DOIPubMedGoogle Scholar
- Santé Publique France. Cas de variole du singe : point de situation au 15 novembre 2022 [cited 2023 Jan 10]. https://www.santepubliquefrance.fr/les-actualites/2022/cas-de-variole-du-singe-point-de-situation-au-15-novembre-2022
- Peñuelas Leal R, Labrandero Hoyos C, Grau Echevarría A, Martínez Domenech Á, Lorca Sprohnle J, Casanova Esquembre A, et al. Dory flop sign in monkeypox: 2 cases. Sex Transm Dis. 2022;49:858–9. DOIPubMedGoogle Scholar
- Pourriyahi H, Aryanian Z, Afshar ZM, Goodarzi A. A systematic review and clinical atlas on mucocutaneous presentations of monkeypox: with a comprehensive approach to all aspects of the new and previous monkeypox outbreaks. J Med Virol. 2022; [Epub ahead of print].PubMedGoogle Scholar
- Eisenstadt R, Liszewski WJ, Nguyen CV. Recognizing minimal cutaneous involvement or systemic symptoms in monkeypox. JAMA Dermatol. 2022;158:1457–8. DOIPubMedGoogle Scholar
- Caldas JP, Valdoleiros SR, Rebelo S, Tavares M. Monkeypox after occupational needlestick injury from pustule. Emerg Infect Dis. 2022;28:2516–9. DOIPubMedGoogle Scholar
Figure
Cite This ArticleOriginal Publication Date: March 14, 2023
Table of Contents – Volume 29, Number 4—April 2023
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Souheil Zayet, Department of Infectious Disease, Nord Franche-Comté Hospital, 100 Route de Moval, 90400 Trevenans, France
Top