Volume 30, Number 6—June 2024
Synopsis
Electronic Health Record–Based Algorithm for Monitoring Respiratory Virus–Like Illness
Noelle M. Cocoros , Karen Eberhardt, Vu-Thuy Nguyen, Catherine M. Brown, Alfred DeMaria, Lawrence C. Madoff, Liisa M. Randall, and Michael Klompas
, Karen Eberhardt, Vu-Thuy Nguyen, Catherine M. Brown, Alfred DeMaria, Lawrence C. Madoff, Liisa M. Randall, and Michael Klompas
Figure 2
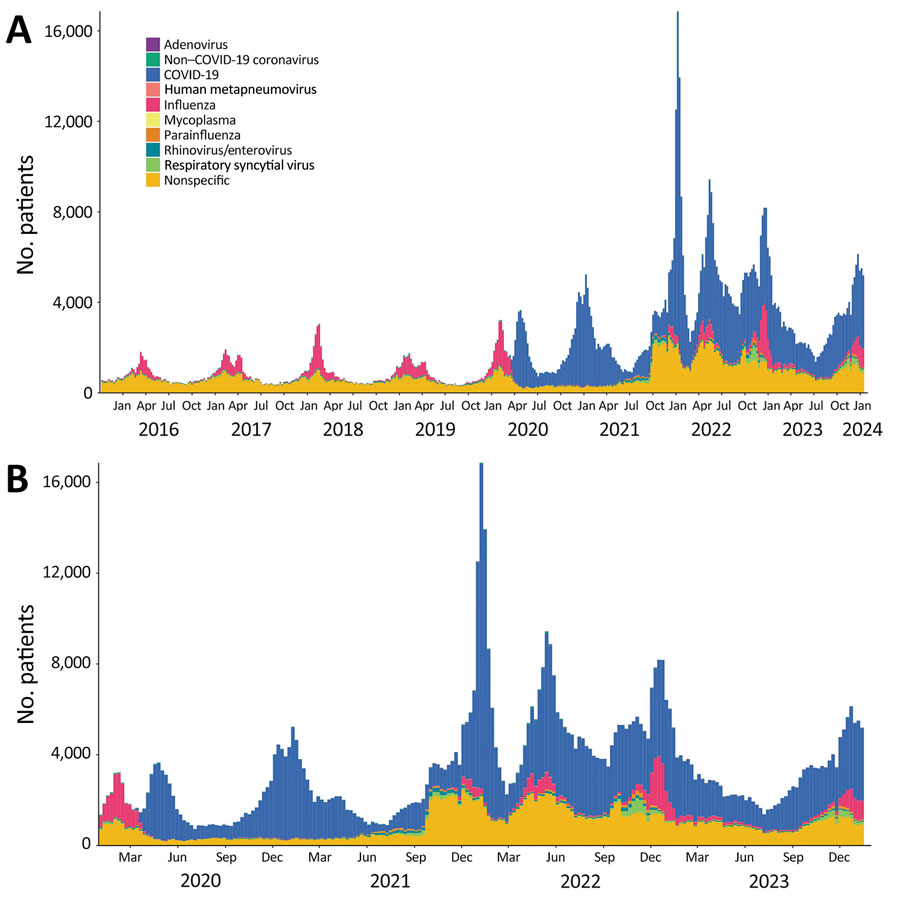
Figure 2. Numbers of patients that met the requirements for the RAVIOLI algorithm for monitoring respiratory virus–like illness, by pathogen category and week, Massachusetts, USA, October 2015–January 2024. A) October 2015–January 2024; B) January 2020–January 2024. Within each virus-specific category are counts of positive test results and diagnosis codes with a positive predictive value (PPV) ≥10% for that specific pathogen. The nonspecific category includes diagnosis codes with a PPV of ≥10% for any positive respiratory viral assay but PPV of <10% for any specific respiratory virus and includes measured fever >100°F.
Page created: April 11, 2024
Page updated: May 22, 2024
Page reviewed: May 22, 2024
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.