Volume 31, Number 1—January 2025
Online Report
Research and Development of Medical Countermeasures for Emerging Infectious Diseases, China, 1990–2022
Cite This Article
Citation for Media
Abstract
Since the severe acute respiratory syndrome outbreak in 2003, China has invested substantial efforts in promoting scientific and technological advances for medical countermeasures against high-threat pathogens. The examination of China’s landscape identifies progress and gaps in research and development (R&D) and also highlights management and regulatory issues that should be of concern to other countries. Our study examined the current state of R&D of medical countermeasures in China during 1990–2022. The findings showed a robust and diversified pipeline responding quickly to disease outbreaks and policy changes. However, proactive and highly innovative candidates are limited, and a large proportion of vaccines and drugs stagnate at the early development stage. A paradigm shift involving a preemptive R&D agenda and persistent investment, innovative technology development, and accelerated research translation is urgently needed to prepare for the next pandemic.
The unprecedented outbreaks of mpox and COVID-19 reminded the world that the global research and development (R&D) system was unprepared to tackle emerging infectious diseases (EIDs) ahead of outbreaks. A collective approach for developing effective medical countermeasures, including vaccines, therapeutic drugs, and diagnostic devices, is urgently needed to avert large-scale crises and strengthen global health security (1). As a high-risk country for indigenous and imported pathogens, China has put substantial effort into promoting scientific and technological advances for medical countermeasures with regulatory reforms and strategies (2). Improvements in China’s ability to detect, prevent, and control EIDs are of global interest. However, because of lacking or insufficient data sources, information on the progress of R&D in China is limited (3,4). To evaluate to what extent the current pipeline addresses EIDs with pandemic and epidemic potential, our study comprehensively analyzed publicly available information on R&D efforts in China, including the development pipeline, clinical trials, and R&D activities during 1990–2022.
Disease Scope
The scope of EIDs included in this analysis is mainly based on the R&D Blueprint of the World Health Organization (WHO) (5). As a global strategy and plan of action, the Blueprint prioritized a list of pathogens that will most likely cause the next epidemic and require proactive R&D activities (5). We included all pathogens identified or discussed in the Blueprint and others recognized in peer-reviewed literature as posing public health risks to China since 1990, except those with a wide range of R&D pipelines, funding flows, or global elimination or eradication programs (i.e., HIV/AIDS, malaria, tuberculosis, viral hepatitis, COVID-19, smallpox, and Guinea worm disease). A total of 63 diseases were identified and grouped into 3 categories: viral, bacterial, and parasitic and other groups (Appendix).
Search Strategy and Eligibility
We identified all originally China-developed vaccine, therapeutic, and diagnostic candidates for human use and phase I–III clinical trials during January 1, 1990–September 20, 2022, on the PharmCube and Yaozhi databases. Those 2 databases cover the most comprehensive information of its kind on the entire lifecycle of pharmaceutical products developed in China from multiple sources, such as the National Medical Products Administration, Center for Drug Evaluation, and Chinese Clinical Trial Registry, and have been widely used by industry, academia, and government for pharmaceutical analysis (6–9). We retrieved the profiles of candidates and clinical trials by defining pathogen or disease name, related MeSH terms, or cataloged synonyms. We classified candidates into the following types: pathogen/disease, development phase, product type, technology platform, developer type, R&D type, and regulatory pathway. We classified clinical trials by pathogen/disease, study phase, study type, location, sponsor and collaborator type, and first posted year. Two reviewers (J.M. and Y.Y.) manually verified data with parameters of candidate and pathogen names across the Center for Drug Evaluation Annual Drug Review Report, Chinadrugtrials.org.cn, ClinicalTrials.gov, Pharmsnap database, company and WHO websites, media and press releases, and other sources. A third researcher (Y.M.) reviewed discordant information until a consensus was reached.
To capture the portfolio and public funding of basic research, we also searched for research projects funded by the National Natural Science Foundation of China (NSFC) on its Big Data Knowledge Management Service Portal during January 1, 1990–December 31, 2019 (when the portal was updated). The funding was converted into US dollars using the exchange rate for the year of award from the International Monetary Fund. By searching government websites and PKUlaw (China’s legal and normative database), we systematically collected national-level policy documents related to EID R&D, covering laws, regulations, procedures, plans, strategies, norms, and guidelines.
Eligible candidates included vaccines, innovative therapeutics, and diagnostic devices initially developed for EIDs by developers in China. We excluded those developed by foreign enterprises but licensed to or manufactured in China, biosimilar drugs, improved new drugs, and generic drugs. We deemed clinical trials eligible if they were registered for diagnosis, treatment, prevention, or control of EIDs by developers in China. We excluded trials applied by foreign developers but carried out in China. We included NSFC projects if they specifically mentioned in research objectives or expected outcomes the advancement of knowledge and new technologies for detecting, preventing, controlling, or treating EIDs. We excluded projects related to EIDs but outside the scope of medical countermeasures (i.e., projects focused on etiology, physiology, ecology, or public health). We identified policies if they explicitly mentioned in the theme or content accelerating or promoting R&D for diagnosing, treating, preventing, or controlling EIDs or in the context of public health emergencies.
Overview of EID Pipeline in China
As of September 20, 2022, at least 118 vaccines, 52 therapeutics, and 285 diagnostic devices were in China’s pipeline, covering a total of 36 EIDs (Appendix). Diseases with the most medical countermeasure candidates were dengue fever (49 candidates), enterovirus A71 infection (43 candidates), and rabies (35 candidates). In contrast, Crimean-Congo hemorrhagic fever, Rift Valley fever, Marburg virus disease, and African trypanosomiasis were the least represented diseases; only 1 candidate each was under early development.
Collectively, 41.5% of vaccines and 36.5% of therapeutics were in the preclinical phase, substantially more than were in phase I–III clinical trials (18.6% of vaccines and 23.1% of therapeutics). Of the 317 medical countermeasures approved for market, 249 (78.5%) were diagnostic devices, largely held by dengue fever–focused devices approved for export (44 of 45); approved vaccines (14.8%, 47) and therapeutics (6.6%, 21) were represented by Japanese encephalitis (11 vaccines), shigellosis, necrotizing cellulitis, and necrotizing fasciitis (5 drugs each). The WHO also prequalified 2 of the approved vaccines: the live-attenuated Japanese encephalitis vaccine (SA 14-14-2) in 2013 and the inactivated influenza (H1N1) vaccine (split virion) in 2015 (10).
R&D Characteristics of EID Candidates
Figure 1

Figure 1. Pipeline of medical countermeasures for emerging infectious diseases by technology platform, China, 1990–2022. A) Distribution of medical countermeasures by technology platform; B) distribution of vaccines and therapeutics by technology platform...
For the technology platform, inactivated vaccines (69.8%) and immunological diagnostics (60.0%) accounted for the largest percentages of each portfolio (Figure 1, panel A). Chemical and biologic drugs contributed an equal share of therapeutic portfolio, 34.6%. However, approved drugs largely consisted of traditional Chinese medicines (13 of 21) (Figure 1, panel B). The most advanced therapeutic candidate was a bispecific antibody for rabies (GR1801) in phase III clinical trial. It has demonstrated broad-spectrum neutralizing activity against naturally occurring rabies virus glycoprotein and pseudo-typed rabies virus, and trials were expected to be completed by July 2024 (ClinicalTrials.gov no. NCT05846568) (11). Several candidates based on emerging technologies (e.g., mRNA vaccine, monoclonal antibody) were at preclinical and phase I stages.
Figure 2
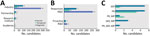
Figure 2. Pipeline of medical countermeasures for emerging infectious diseases by developer type, R&D type, and regulatory pathway, China, 1990–2022. Partnership indicates that the candidate was jointly developed by >2...
Assessment of candidate developers showed the key involvement of private industry in developing 78.0% of vaccines (92 candidates), 59.6% of therapeutics (31 candidates), and 98.9% of diagnostics (282 candidates) (Figure 2, panel A). The vaccine and therapeutic pipelines were concentrated in 2 pharmaceutical companies (Sino Biopharmaceutical [https://www.sinobiopharm.com] and Jiangsu Kanion Pharmaceutical [https://kanion.en.made-in-china.com]), accounting for 27.9% of vaccines and 13.2% of therapeutics. In contrast, the diagnostic pipeline is widely distributed; 81 companies were working on >1 diagnostic product for EIDs. Comparing the timeline between the occurrence of disease in China and the earliest R&D activity, ≈90% of candidates of each medical countermeasure type were responsively developed after the onset of diseases (Figure 2, panel B). A few candidates were proactively initiated in case of the appearance and transmission of influenza (H1N1), yellow fever, Ebola, Marburg virus, and West Nile virus. For regulatory pathway, the Ebola recombinant adenovirus vector-based vaccine (Ad5-EBOV) was the only product that received priority review, special examination review, and major program support simultaneously (Figure 2, panel C). It became the first domestically developed product approved for strategic national stockpile under emergency use authorization (12). Other candidates granted the largest number of expedited regulatory designations were vaccines for influenza (H7N9) (5 candidates) and enterovirus A71 infection (3 candidates).
Trends of R&D Activities for EIDs
Figure 3

Figure 3. Titles and corresponding years of policy documents issued by government of China regarding research and development activities on emerging infectious diseases, 1990–2022.
During 1990–2019, China invested a total of US $26.3 million in 313 NSFC research projects to promote knowledge and develop technologies and products for detecting, preventing, and treating EIDs (Figure 3). The largest batch (33.5%, US $8.8 million) was in 2015, which included the funding of medical countermeasure development against Ebola virus disease (27.0%, US $7.1 million). The number of trials entering all stages of clinical development increased after 2005; the average annual growth rate was 59.8%. The sharp decline in 2015 could be explained by the self-inspection and verification process conducted by the National Medical Products Administration the same year, in which a large number of clinical trial applications were withdrawn or rejected to ensure data authenticity and integrity in regulatory filings (13). The trends of NSFC funding and projects were consistent with the timing of a series of strategic plans and policies on promoting new technology and product development for major EIDs. After 2017, momentum gradually decreased until it reached 2011 levels in 2019, indicating a swift deviation of public interest in EID research in the postoutbreak period.
Figure 4
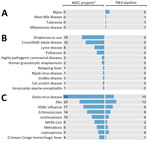
Figure 4. Distribution of NSFC projects and R&D pipeline by disease in study of R&D of medical countermeasures for emerging infectious diseases, China, 1990–2022. The figure shows a rough comparison between basic...
To understand the relative intensity of basic and applied research, we roughly compared the number of NSFC projects and R&D pipeline by each EID. The imbalanced distribution highlighted 3 groups of EIDs in need of urgent action: diseases with crucial gaps in basic research (e.g., mpox, West Nile virus, and tularemia) (Figure 4, panel A); diseases with crucial gaps in applied research (e.g., Streptococcus suis, Creutzfeldt-Jakob disease, and Lyme disease) (Figure 4, panel B); and diseases that might enhance translational research from basic to application (e.g., Ebola virus disease, Zika virus, and influenza [H5N1]) (Figure 4, panel C). In addition, of the 63 diseases included in the analysis, 16 have neither basic research nor R&D pipelines according to public data; included in those 16 diseases were Lassa fever and henipavirus disease, both of which were prioritized by the WHO R&D Blueprint (5).
Our study provides current and comprehensive country-level evidence on medical countermeasure development for EIDs in China. Since the lessons learned from severe acute respiratory syndrome, China has attached great importance to public health preparedness and response capacity-building. The successful development of Ebola vaccine indicates a robust national commitment and governance of R&D forces in response to global public health emergency. The pipeline, research, and clinical activities responded quickly to public policies and disease outbreaks, indicating fundamental R&D capacity and infrastructure to meet environmental changes. However, despite substantial efforts achieved over 3 decades, a major and persistent gap remains in basic research, product development, and clinical activities for most EIDs. Cutting-edge candidates are few, and most active candidates stagnated at early development phase. To better prepare for future outbreaks, urgent actions are needed to increase early R&D planning and investment in EIDs, enhance innovative technology platform development, and promote translation research from basic discovery into clinical advance.
Because the emergence of EIDs is challenging to predict and usually confined to limited geographic settings, the global R&D pipeline has lacked appropriate investment until a new pathogen shows explosive growth (14). Pharmaceutical companies have little market incentive to invest resources in developing medical countermeasures that are unlikely to yield comparable investment return versus other opportunities in a short time (15). That persistent underinvestment leads to the absence of available products to meet population need at the time of outbreak, which in turn causes increased health burden, economic losses, and social instability (16). Compared with oncology, the R&D hotspot in China, the pipeline for medical countermeasures for EIDs has a huge gap in terms of scale and vitality; the total number of oncology therapeutics (359) in 2020 was 6.9 times higher than the total number of EID therapeutics (52), and the proportion of candidates in phase I–III trials (71.9%) was >3.1 times that of candidates for EIDs (23.1%) (17). For diseases posing a major global and national threat (e.g., mpox, Lassa fever, and Streptococcus suis), the current pipeline is missing >1 of the basic, translational, and applied research stages. Most NSFC projects and candidate development were launched responsively after outbreak of disease, resulting in a funding cycle too short to produce noteworthy basic discoveries and technology breakthroughs. Our findings are consistent with studies worldwide that reported patterns of insufficient and unsustainable funding, responsive R&D activities, and weak correlation between disease burden and research investment (3,18). To overcome market failures, governments should take responsibility for developing national plans and strategies to accelerate R&D and stockpiling of medical countermeasures with persistent and proactive inputs before the next pandemic (15). Many developed countries, such as the United States, United Kingdom, and Australia, have already established R&D preparedness and response plans for tackling high-risk and unknown pathogens (19–21). Establishing a country-level R&D agenda could provide a cohesive framework for defining critical gaps, focusing on leading technology development, and allocating funding and resources to the highest-priority pathogens on the basis of health and R&D needs. Through the development of medical countermeasures, countries can also take advantage of their own scientific, technological, and innovative strengths for expanding into global markets. This opportunity has been evidenced in China’s mass development of diagnostic devices for dengue fever, which are partly associated with the mature technology and production capacity advantage of domestic industry, as well as by substantial demand from neighboring countries for cross-border screening and virological surveillance (22,23).
Although the current portfolio covers a range of technical routes, candidates from emerging biotechnologies are few, and licensed products mainly depend on conventional inactivated vaccines and traditional Chinese medicines. Those techniques were supported by well-understood safety profiles, mature technology, and ease of production (24,25). However, given the unpredictable, evolving, and highly contagious natures of EIDs, platform-based technology and prototype-based research approaches must be built for a more rapid and effective response to future outbreaks (26). For example, the platform-based technology of the mRNA and viral vector vaccine is designed to assemble genetic material coding into the platform backbone (e.g., a synthetic RNA or viral vector) for inducing immunity once the virus’s genetic information is identified (27,28). This process can achieve last-mile innovation of medical countermeasures against multiple pathogens and enable large-scale production with minimal changes to development, manufacturing, and quality control processes (15,29). For instance, the mRNA-1273 vaccine for COVID-19 (Moderna, https://www.modernatx.com) took only 66 days from gene sequencing to initiation of the first phase I clinical trial (30). It achieved the fastest speed in vaccine development history with proven effectiveness at preventing illness (31). In addition, prototype-based research can also accelerate product development by filling research gaps of viruses of related families prospectively (32). For instance, by leveraging knowledge gained from dengue, West Nile virus, and other flaviviruses, researchers rapidly developed animal models, immunogenicity assays, and vaccine designs against Zika virus when the outbreak started (26).
Our findings also highlight areas that might enhance translation from basic science to clinical application. Some EIDs (e.g., Ebola and Zika virus) are intrinsically difficult to translate because of the inability to recruit sufficient numbers of infected persons as participants. Historically, efficacy trials for severe acute respiratory syndrome and Zika virus vaccines were not completed before the pandemic/epidemic ended (33,34). In this situation, early phase I and II candidates and overseas clinical trial partners should be established in advance to quickly promote the start of phase III clinical trials in the most affected areas during emergencies (32). Another reason for the fragmentation between basic and applied research could be the lack of communication and collaboration among the R&D community (35). Although the current pipeline involves a mix of industry–research institute, industry–academia, industry–industry, and research institute–research institute partnerships, >89.0% of medical countermeasures were developed by individual companies. The high costs of late-stage product development, particularly those related to long-term clinical trials, manufacturing, and commercialization, are likely to result in market failure of financial returns from EID medical countermeasures (36). To cross the ever-widening gap in translational research, functional interaction and coordination mechanisms, including innovation-focused grants, should exist among funding agencies, academia, research institutes, and industry (37).
Our analysis is mainly limited by scarce publicly available data sources. Although great efforts were made to ensure this analysis was as complete as possible and comparable to global-level assessments, data availability and quality varied substantially across databases, diseases, medical countermeasure types, and research activities. Because of data availability, national investment in major national research programs (such as the Major National Scientific Research Programs and the National Key Scientific Research Plans) and direct institutional funding from academia and nonprofit institutions were not included in the public funding analysis, which might underestimate China’s overall public R&D efforts on EIDs. Many companies could discontinue candidate development without publicly announcing the decision and being captured by the database. This landscape assessment should be regarded as a snapshot at the time of its creation. As more information and data become available, the scale and vitality might change.
Our study shows a vibrant and diversified R&D pipeline in China, which has the fundamental capacity and infrastructure to respond rapidly to public policies and disease outbreaks. However, medical countermeasures for most EIDs are insufficient or lacking. Conventional technical routes remain the main focus of development; little emphasis is placed on highly innovative technology and proactive candidates. The pipeline faces the risk of drying up, especially when a large proportion of vaccines and drugs cumulate in the early development phase. Our findings serve as a resource for ongoing portfolio management and draw attention to areas in immediate need of increased support. We hope to highlight the significance of establishing a preemptive R&D agenda and investment, promoting innovative technology development, and enhancing translation research that could be conducive to other countries.
Ms. Ma is a lecturer in the School of Public Administration of the Southwestern University of Finance and Economics. Her research interests focus on improving research and development and access to global public goods for health, especially in the area of emerging infectious diseases.
Acknowledgments
Our study was supported by the National Natural Science Foundation of China (nos. 7207040929 and 72361127504).
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the Peking University with which the authors are affiliated.
References
- Fauci AS, Folkers GK. Pandemic preparedness and response: lessons from COVID-19. J Infect Dis. 2023;228:422–5. DOIPubMedGoogle Scholar
- Han M, Gu J, Gao GF, Liu WJ. China in action: national strategies to combat against emerging infectious diseases. Sci China Life Sci. 2017;60:1383–5. DOIPubMedGoogle Scholar
- Policy Cures Research. Landscape of emerging infectious disease research and development: from pandemic response to pandemic resilience [cited 2023 Oct 20]. https://policy-cures-website-assets.s3.ap-southeast-2.amazonaws.com/wp-content/uploads/2022/06/16191104/2022-G-FINDER-EID-Report.pdf
- Røttingen JA, Regmi S, Eide M, Young AJ, Viergever RF, Ardal C, et al. Mapping of available health research and development data: what’s there, what’s missing, and what role is there for a global observatory? Lancet. 2013;382:1286–307. DOIPubMedGoogle Scholar
- Mehand MS, Al-Shorbaji F, Millett P, Murgue B. The WHO R&D Blueprint: 2018 review of emerging infectious diseases requiring urgent research and development efforts. Antiviral Res. 2018;159:63–7. DOIPubMedGoogle Scholar
- Li G, Liu Y, Hu H, Yuan S, Zhou L, Chen X. Evolution of innovative drug R&D in China. Nat Rev Drug Discov. 2022;21:553–4. DOIPubMedGoogle Scholar
- Yue J, Liu Y, Zhao M, Bi X, Li G, Liang W. The R&D landscape for infectious disease vaccines. Nat Rev Drug Discov. 2023;22:867–8. DOIPubMedGoogle Scholar
- Liu Y, Zhang N, Xie C, Jiang Y, Qin Y, Zhou L, et al. Evolution of drug regulations and regulatory innovation for anticancer drugs in China. Acta Pharm Sin B. 2022;12:4365–77. DOIPubMedGoogle Scholar
- Zhang Y, Naci H, Wagner AK, Xu Z, Yang Y, Zhu J, et al. Overall survival benefits of cancer drugs approved in China from 2005 to 2020. JAMA Netw Open. 2022;5:
e2225973 . DOIPubMedGoogle Scholar - World Health Organization. Prequalified vaccines [cited 2023 Oct 20]. https://extranet.who.int/prequal/vaccines/prequalified-vaccines
- Long C, Wang W, Hao X, Yu C, Feng Y, Tu C, et al. Development of a novel bispecific antibody GR1801 for rabies. J Med Virol. 2023;95:
e29016 . DOIPubMedGoogle Scholar - Mathebula L, Ndwandwe DE, Pienaar E, Wiysonge CS. Effects of vaccines in protecting against Ebola virus disease: protocol for a systematic review. BMJ Open. 2019;9:
e029617 . DOIPubMedGoogle Scholar - Shao L, Xu L, Li Q, Chakravarthy R, Yang Z, Kaitin KI. Regulatory watch: Innovative drug availability in China. Nat Rev Drug Discov. 2016;15:739–40. DOIPubMedGoogle Scholar
- Gopinathan U, Peacocke E, Gouglas D, Ottersen T, Røttingen JARR. R&D for Emerging Infectious Diseases of Epidemic Potential: Sharing Risks and Benefits Through a New Coalition. Infectious Diseases in the New Millennium. 2020;82:137–65. DOIGoogle Scholar
- Torreele E, Wolfe D, Kazatchkine M, Sall A, Ruxrungtham K, Fitchett JRA, et al. From private incentives to public health need: rethinking research and development for pandemic preparedness. Lancet Glob Health. 2023;11:e1658–66. DOIPubMedGoogle Scholar
- Shang Y, Li H, Zhang R. Effects of pandemic outbreak on economies: evidence from business history context. Front Public Health. 2021;9:
632043 . DOIPubMedGoogle Scholar - Li G, Qin Y, Xie C, Wu YL, Chen X. Trends in oncology drug innovation in China. Nat Rev Drug Discov. 2021;20:15–6. DOIPubMedGoogle Scholar
- Head MG, Brown RJ, Newell ML, Scott JAG, Batchelor J, Atun R. The allocation of USdollar;105 billion in global funding from G20 countries for infectious disease research between 2000 and 2017: a content analysis of investments. Lancet Glob Health. 2020;8:e1295–304. DOIPubMedGoogle Scholar
- Australia’s National Science Agency. Strengthening Australia’s pandemic preparedness [cited 2023 Oct 20]. https://www.csiro.au/en/work-with-us/services/consultancy-strategic-advice-services/csiro-futures/health-and-biosecurity/strengthening-australias-pandemic-preparedness
- National Institute of Allery and Infectious Disease. NIAID pandemic preparedness plan [cited 2023 Oct 20]. https://www.niaid.nih.gov/sites/default/files/pandemic-preparedness-plan.pdf
- Noad RJ, Simpson K, Fooks AR, Hewson R, Gilbert SC, Stevens MP, et al. UK vaccines network: Mapping priority pathogens of epidemic potential and vaccine pipeline developments. Vaccine. 2019;37:6241–7. DOIPubMedGoogle Scholar
- Liu Q, Xu W, Lu S, Jiang J, Zhou J, Shao Z, et al. Landscape of emerging and re-emerging infectious diseases in China: impact of ecology, climate, and behavior. Front Med. 2018;12:3–22. DOIPubMedGoogle Scholar
- Brisse M, Vrba SM, Kirk N, Liang Y, Ly H. Emerging concepts and technologies in vaccine development. Front Immunol. 2020;11:
583077 . DOIPubMedGoogle Scholar - Yang Y, Tian K, Bai G, Zhu X, Yang Y, Yu X, et al. Health technology assessment in traditional Chinese medicine in China: current status, opportunities, and challenges. Glob Health J. 2019;3:89–93. DOIGoogle Scholar
- Marston HD, Paules CI, Fauci AS. The critical role of biomedical research in pandemic preparedness. JAMA. 2017;318:1757–8. DOIPubMedGoogle Scholar
- Bloom DE, Black S, Rappuoli R. Emerging infectious diseases: A proactive approach. Proc Natl Acad Sci U S A. 2017;114:4055–9. DOIPubMedGoogle Scholar
- Adalja AA, Watson M, Cicero A, Inglesby T. Vaccine platform technologies: a potent tool for emerging infectious disease vaccine development. Health Secur. 2020;18:59–60. DOIPubMedGoogle Scholar
- Monrad JT, Sandbrink JB, Cherian NG. Promoting versatile vaccine development for emerging pandemics. NPJ Vaccines. 2021;6:26. DOIPubMedGoogle Scholar
- Huang Q, Zeng J, Yan J. COVID-19 mRNA vaccines. J Genet Genomics. 2021;48:107–14. DOIPubMedGoogle Scholar
- Tseng HF, Ackerson BK, Luo Y, Sy LS, Talarico CA, Tian Y, et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat Med. 2022;28:1063–71. DOIPubMedGoogle Scholar
- Cassetti MC, Pierson TC, Patterson LJ, Bok K, DeRocco AJ, Deschamps AM, et al. Prototype pathogen approach for vaccine and monoclonal antibody development: a critical component of the NIAID plan for pandemic preparedness. J Infect Dis. 2023;227:1433–41. DOIPubMedGoogle Scholar
- Del Rio C, Malani P. Translating science on COVID-19 to improve clinical care and support the public health response. JAMA. 2020;323:2464–5. DOIPubMedGoogle Scholar
- Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 vaccines at pandemic speed. N Engl J Med. 2020;382:1969–73. DOIPubMedGoogle Scholar
- Fears R, van der Meer JW, ter Meulen V. Translational medicine policy issues in infectious disease. Sci Transl Med. 2010;2:14cm2. DOIPubMedGoogle Scholar
- Schäferhoff M, Zimmerman A, Diab MM, Mao W, Chowdhary V, Gill D, et al. Investing in late-stage clinical trials and manufacturing of product candidates for five major infectious diseases: a modelling study of the benefits and costs of investment in three middle-income countries. Lancet Glob Health. 2022;10:e1045–52. DOIPubMedGoogle Scholar
- Seyhan A. Lost in translation: the valley of death across preclinical and clinical divide – identification of problems and overcoming obstacles. Transl Med Commun. 2019;4:18. DOIGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: December 17, 2024
Table of Contents – Volume 31, Number 1—January 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Yangmu Huang, School of Public Health, Peking University, No.38, Xueyuan Rd, Haidian District, Beijing, 100191, China
Top