Volume 31, Number 10—October 2025
Research Letter
Increased Rates of Purpureocillium lilacinum Mold among Laboratory Culture Results, United States
Cite This Article
Citation for Media
Abstract
Purpureocillium lilacinum, a common environmental mold and bionematicide, can cause human infections. At a major US commercial laboratory during March 2019–February 2025, P. lilacinum culture rates increased; rates were highest in the South Atlantic and Pacific states. Nonculture-based diagnostic tools such as microscopy may help identify and confirm clinical infection earlier.
Purpureocillium lilacinum (formerly Paecilomyces lilacinus) is a naturally occurring filamentous fungus that is common in the environment, particularly in soil and decaying vegetation (1). Two strains of P. lilacinum registered in 2005 and 2021 are used as agricultural bionematicides in the United States (2,3). The fungus rarely causes human infection but can cause hyalohyphomycosis, an infection with varied clinical soft-tissue, ocular, or pulmonary manifestations. Infection most frequently affects immunocompromised persons but can also occur in immunocompetent persons. Mortality rates can reach 20% (1).
P. lilacinum infection is clinically indistinguishable from other mold infections, and the organism resembles other molds on cytology, histopathology, and culture, potentially leading to misidentification and to delayed or inappropriate treatment (1). P. lilacinum is intrinsically resistant to amphotericin B and can be correlated with poorer treatment outcomes (1,4).
Worldwide, clinical characteristics and outcomes of 101 P. lilacinum infections have been described, 31 of which were from the United States, but epidemiology of the infection in the United States is poorly understood (1). We explored P. lilacinum culture data from a large national commercial laboratory to describe this organism in the United States.
We used data from the Centers for Disease Control and Prevention’s National Syndromic Surveillance Program (NSSP) (https://www.cdc.gov/nssp/index.html), which collects data from Labcorp (https://www.labcorp.com), a major national commercial laboratory network. Labcorp transmits test orders and results for all reportable diseases in the United States to NSSP. Although P. lilacinum infection is not reportable to public health authorities, NSSP receives data on all fungal cultures performed at Labcorp because other fungal diseases are reportable (5). We identified culture results for P. lilacinum ordered during March 1, 2019 (earliest available data) through February 28, 2025.
We examined demographic characteristics, geographic location of submitting provider’s state (US Census division), specialty or setting of the ordering healthcare provider, specimen type, and time from test order to culture result. Unique patient identifiers were unavailable; therefore, we conducted analyses at the test-result level.
Figure
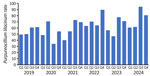
Figure. Rates of Purpureocillium lilacinum mold among laboratory culture results, United States. Graph shows P. lilacinumcultures per 100,000 fungal cultures by year and quarter during March 2019–February...
We identified 1,180 P. lilacinum cultures (Table; Appendix Figure 1). Rates of P. lilacinum per 100,000 fungal cultures per year increased from 56.6 in 2019 to 74.3 in 2024 and peaked at >90 in the third quarter of 2024 (Figure). Overall, male persons (68.8/100,000 population) and persons >65 years of age (89.7/100,000 population) had the highest culture rates. By US Census division, the South Atlantic (110.6/100,000 population) and Pacific (100.3/100,000 population) divisions had the highest rates. Most (52%) P. lilacinum cultures were ordered from hospital settings. Specimen type was available for 57% of cultures, among which respiratory specimens were most common (38%). The median time from collection to result was 23 (interquartile range 15.0–33.0) days.
Those commercial laboratory data suggest a recent increase in P. lilacinum cultures in the United States and a wide geographic distribution. Higher rates among male persons and older persons align with a previous study of P. lilacinum infections (1). The long time (>3 weeks) for culture growth and identification for this mold might lead to diagnostic delays and potentially inappropriate treatment (1,4).
The South Atlantic and Pacific Census divisions had substantially higher P. lilacinum culture rates than other regions of the United States. The high rates in the Pacific region could reflect a substantial uptick in cultures from that area during 2024–2025, including 60 cultures from a single facility that was the subject of a public health investigation (6). That event represented a pseudo-outbreak from environmental contamination rather than a true clinical outbreak, which is a rare occurrence. A previous P. lilacinum outbreak was linked to contaminated skin lotion (7). Two strains of P. lilacinum are used in the United States as agricultural bionematicides, PL251 registered in 2005 and PL11 registered in 2021 (2,3). Use of those bionematicides could possibly contribute to increased environmental presence and culture contamination during collection or in laboratories. Internationally, at least 1 case of subcutaneous P. lilacinum infection has been reported in association with bionematicide use (8). We could not assess environmental exposures in patients from whom the cultures in our study were derived; more data are needed on potential P. lilacinum environmental sources and their correlation with clinical culture positivity and infection risk.
Without clinical data, we were unable to determine patients’ underlying medical conditions and whether cultures represented true infection versus colonization. The most common specimen source was the respiratory tract, which can be colonized with various molds. Furthermore, nearly half of cultures were missing specimen type information, likely skewing our results; however, another study of confirmed infections found that skin was the most common infection site (1). Last, our data are a convenience sample and might not necessarily represent the entire US population.
In summary, mold infections generally are associated with substantially delayed and missed diagnoses (9). Further investigations are needed to understand the increased P. lilacinum culture rates, including examining bionematicide use, environmental changes, and clinical effects. Because P. lilacinum culture rates appear to be increasing, clinicians could consider nonculture-based diagnostic tools, such as microscopy (Appendix Figure 2), to help identify and confirm clinical infection earlier.
Dr. Smith is an epidemiologist with the Mycotic Diseases Branch, Division of Foodborne, Waterborne, and Environmental Diseases, National Center for Zoonotic and Emerging Infectious Diseases, Centers for Disease Control and Prevention. His main research interests include environmental molds, fungal neglected tropical diseases, and antifungal stewardship.
Acknowledgments
The authors thank Stephanie Dietz for assistance with NSSP data.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Department of Agriculture.
References
- Sprute R, Salmanton-García J, Sal E, Malaj X, Ráčil Z, Ruiz de Alegría Puig C, et al.; FungiScope® ECMM/ISHAM Working Group. Invasive infections with Purpureocillium lilacinum: clinical characteristics and outcome of 101 cases from FungiScope® and the literature. J Antimicrob Chemother. 2021;76:1593–603. DOIPubMedGoogle Scholar
- US Environmental Protection Agency. Registration decision for the new active ingredient Purpureocillium lilacinum strain PL11 [cited 2025 Apr 1]. https://www.regulations.gov/document/EPA-HQ-OPP-2016-0079-0013
- US Environmental Protection Agency. Paecilomyces species PC Codes 115002, 028826, and 115003 Interim registration review decision case number 6047 [cited 2025 Apr 1]. https://www.regulations.gov/document/EPA-HQ-OPP-2012-0403-0011
- Castelli MV, Alastruey-Izquierdo A, Cuesta I, Monzon A, Mellado E, Rodriguez-Tudela JL, et al. Susceptibility testing and molecular classification of Paecilomyces spp. Antimicrob Agents Chemother. 2008;52:2926–8. DOIPubMedGoogle Scholar
- Centers for Disease Control and Prevention. Reportable fungal diseases by state [cited 2025 Sep 12]. https://www.cdc.gov/fungal/php/case-reporting/index.html
- Centers for Disease Control and Prevention. Fungi faux pas: investigating a Purpureocillium lilacinum skin infection cluster—Washington, 2024 [cited 2025 Aug 20]. https://www.cdc.gov/eis-conference/php/media-resources/purpureocillium-lilacinum-skin-infection.html
- Orth B, Frei R, Itin PH, Rinaldi MG, Speck B, Gratwohl A, et al. Outbreak of invasive mycoses caused by Paecilomyces lilacinus from a contaminated skin lotion. Ann Intern Med. 1996;125:799–806. DOIPubMedGoogle Scholar
- Zheng C, Li W, Gao Z, Yu Q, Yang L. Deep cutaneous fungal infection in an immunocompetent individual caused by a biological pesticide: a rare case report. BMC Infect Dis. 2025;25:341. DOIPubMedGoogle Scholar
- Caudron de Coquereaumont G, Couchepin J, Perentes JY, Krueger T, Lovis A, Rotman S, et al. Limited index of clinical suspicion and underdiagnosis of histopathologically documented invasive mold infections. Open Forum Infect Dis. 2021;8:ofab174. DOIGoogle Scholar
Figure
Table
Cite This ArticleOriginal Publication Date: September 22, 2025
Table of Contents – Volume 31, Number 10—October 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Dallas J. Smith, Centers for Disease Control and Prevention, 1600 Clifton Rd NE, Mailstop H24-11, Atlanta, GA 30329-4018, USA;rhq8@cdc.gov
Top