Volume 31, Number 3—March 2025
Synopsis
Candida auris Outbreak and Epidemiologic Response in Burn Intensive Care Unit, Illinois, USA, 2021–2023
Figure 3
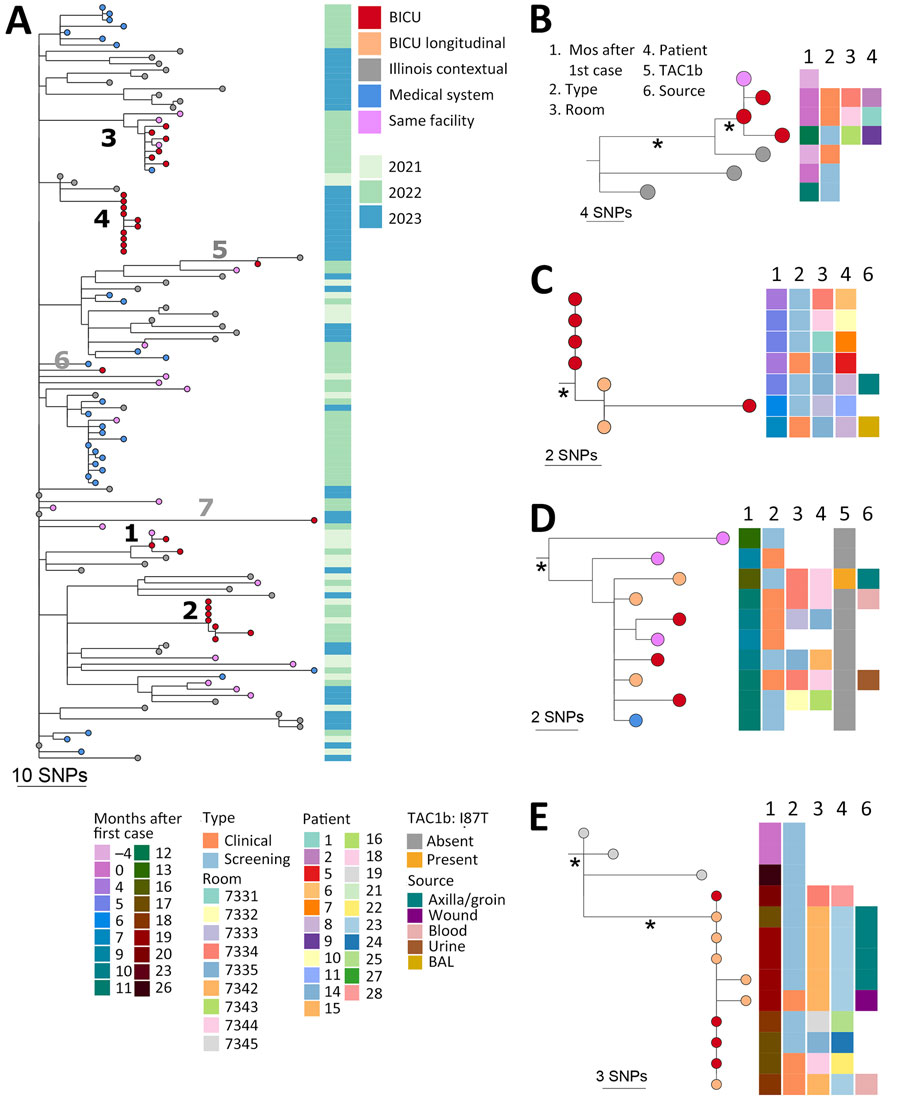
Figure 3. Genomic analysis of outbreak and contemporaneous contextual Candida auris isolates in outbreak of C. auris in BICU, Illinois, USA, 2021–2023. A) Neighbor-joining SNP-based phylogenetic tree of sequences from BICU isolates, isolates collected from the same facility or another facility within the medical system, and publicly available Illinois sequences collected in 2021–2023. Facility source for 31 of 43 Illinois contextual sequences was confirmed as not within the BICU medical system. The facility source of the remaining 12 isolate sequences was not known. Branch lengths are SNP distances. Isolate collection year is indicated in metadata column to the right. Numbers 1–4 indicate branches leading to BICU clusters; numbers 5–7 indicate branches leading to BICU isolates that do not cluster with others. B–E) Subtrees from BICU cluster 1 (B), cluster 2 (C), cluster 3 (D), and cluster 4 (E). Relevant isolate and patient metadata are indicated in the columns to the right of tree tips; key at bottom shows metadata coding for panels B–E. Orange tips indicate isolates collected from the same person. Isolate collection date is shown as months after the first BICU case. Asterisks (*) indicate branches with >95% bootstrap support. Scale bars indicate SNPs. BICU, burn intensive care unit; SNP, single-nucleotide polymorphism.
1These first authors contributed equally to this article.
2These authors contributed equally to this article.