Volume 31, Number 3—March 2025
Dispatch
Outbreak Caused by Multidrug-Resistant Mycobacterium Tuberculosis with Unusual Combination of Resistance Mutations, Northern Argentina, 2006–2022
Cite This Article
Citation for Media
Abstract
To reconstruct transmission chains of the multidrug-resistant tuberculosis Ch strain, which harbors a unique combination of resistance mutations, we analyzed genomes of 25 isolates from 12 patients with diagnosis during 2006–2022 in Chaco Province, Argentina. Amplification of resistance, high mortality rates, and indications of a wider outbreak raise concerns for surveillance programs.
Argentina is considered a mid-incidence country for tuberculosis (TB); 1% of multidrug-resistant (MDR) cases persist in Argentina. The northern province of Chaco, a province with a top 5 TB burden (1), had a low number of MDR TB cases and no prior evidence of local transmission (2). MDR TB can affect patients beyond the well-established risk groups, making clinical suspicion essential where universal drug-susceptibility testing (DST) is unavailable. Whole-genome sequencing (WGS) enables timely and precise molecular drug-resistance profiling, but genotype/phenotype correlations need further research, especially for rapidly emerging resistance to second-line drugs (e.g., bedaquiline and linezolid) (3).
To reconstruct the transmission chains and drug-resistance profiles, we used WGS to analyze an MDR TB outbreak in Resistencia, Chaco Province, Argentina. The study was performed in accordance with the Helsinki Declaration as revised in 2013. The Research Ethics Committee of the Instituto Nacional de Epidemiologia, ANLIS “Dr. Jara,” Buenos Aires, Argentina, approved the project and waived the informed consent requirement (project code YOKOBORI05/2022).
During 2018–2019, our laboratory received 9 MDR M. tuberculosis isolates from 3 patients of Resistencia, Chaco, that had unexpectedly inconsistent PCR-based resistance profiles for rifampin and isoniazid in isolates from the same patient and between 2 patients with close epidemiologic links (Appendix 1; Appendix2). A preliminary genomic analysis showed simultaneous presence of the mutations rpoB_Asp435His, rpoB_His445Asp, fabG1-inhA_t-8c, and katG_Ser315Thr. We studied that possible outbreak because of the unusual combination of mutations, the extended resistance profile, and the critical disease in young patients with no relevant comorbidities (Table 1).
The Mycobacteria Service, Instituto Nacional de Enfermedades Infecciosas, ANLIS “Dr. C. Malbrán,” Buenos Aires, Argentina, the national reference laboratory for TB diagnosis, has kept an MDR genotyping database, representing nationwide cases, since 2003. After intense screening of our databases, on the basis of rifampin and isoniazid molecular resistance patterns; province of origin; epidemiologic link, genotype, or both, we identified 29 candidate isolates from 12 patients. Twenty-four isolates were available for WGS analysis (Appendix 1); we assigned an identification number to each isolate. We performed phenotypic DST when we received the isolates unless otherwise stated (Appendixes 1, 2), and we compared spoligotypes with those in the SITVITEXTED database (Appendix 3).
All patients were residents of Resistencia, except for a patient from the neighboring Corrientes city and a former resident of Resistencia who received their diagnoses in Buenos Aires (Table 1; Appendix 3). Patient 2, a healthcare worker at the hospital where patient 1 was assisted, was the mother of patients 3, 4, and 9. Patient 6 was the granddaughter of patient 5 and frequently visited her friend, patient 10. The remaining epidemiologic links were unknown. Five patients were teenagers at the time of diagnosis (Table 1).
Figure 1

Figure 1. Maximum-likelihood phylogenetic tree of the 24 isolates from the MDR Mycobacterium tuberculosisoutbreak strain Ch, Chaco, Argentina, 2006–2022, analyzed by whole-genome sequencing. Each patient is represented by a colored...
WGS showed a monophyletic group (Figure 1; Appendix 2). We named the clone the Ch strain, and it belonged to lineage 4.1.1 and to the spoligotype international type (SIT) 119 of the X1 family. The highest number of SIT119 clones in the SITVITEXTEND database in the region, without association with MDR, is in Brazil (Appendix 3). The median pairwise single-nucleotide polymorphism distance among the first isolates from each patient was 3 (range 0–6) (Appendix 2), excluding isolate 8.1, which was 15 single-nucleotide polymorphisms (range 12–17) apart from the others. The most ancestral isolate belonged to the index case-patient, whose diagnosis was made in 2006. Despite the patient having no history of TB treatment, that isolate had the 8 resistance mutations common to the cluster, including the double mutations for isoniazid and rifampin (Table 2; Figure 1), suggesting that the outbreak could have been more extended. Patient 3 was probably the source of 3 secondary pre–extensively drug-resistant cases in the second subcluster. Isolates from the patients with the most recent diagnoses (patients 11 and 12) were closer to the first subcluster (Figure 1).
Figure 2
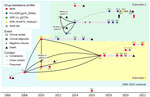
Figure 2. Schematic representations of the timeline and epidemiologic links of the MDR Mycobacterium tuberculosisoutbreak with strain Ch, Chaco, Argentina, 2006–2022. Two subclusters were defined according to the phylogenetic analysis...
The resistance mutations had high World Health Organization (WHO) confidence gradings and were concordant with the phenotypic drug-susceptibility testing results (Table 2), except for ethionamide and ethambutol, as expected (3). Resistance to the second-line injectable drugs was acquired independently in 3 isolates (Figure 1). Two isolates were extensively drug resistant. Isolate 6.4 had a rrl_g2270t mutation, which has recently been associated with linezolid resistance (3), and isolate 10.4 had the loss-of-function mutation Rv0678_144dupC. Resistance to linezolid and cross-resistance to bedaquiline were confirmed by phenotypic methods (Table 2). Instances of clofazimine/bedaquiline resistance were acquired shortly after their administration under strict supervision (Figure 2).
No compensatory mutations were found in rpoC or rpoA. Because both mutations in rpoB are expected to have a mild to high fitness cost (4), their simultaneous presence could constitute a unique compensatory mechanism.
Patient 1 died shortly after diagnosis. The mother of patient 2 had received a TB diagnosis in 2010 but refused treatment and died in 2011. The mother and the brother of patient 6 died in 2013 (Appendix 2). Isolates from those patients were not available. Because isolates 3.2, 5.1, and 6.1 were identical (Figure 1), the other 2 relatives could have acquired their infection from patient 3 (Figure 2), but their epidemiologic link remains unknown. Their close relationship, the contemporaneity, and their fatal outcomes strongly suggest that those patients were part of the outbreak (Figure 2). Patient 9 probably experienced relapse from latency and infected patient 12, who lived at the same address before moving to Buenos Aires. Their relationship remains unclear. Patient 2 administered the medication to her family, including the injectable drugs. Some regimens, especially in the first years of the outbreak, were suboptimal and underwent multiple changes. Reports suggest that empathy from some healthcare providers had been insufficient. Three cohabitants received chemoprophylaxis with isoniazid, and no active disease has been reported (Appendix 2).
The MDR Ch outbreak strain, with its epicenter in Resistencia, Chaco, belonged to the X1, SIT 119 spoligotype, which is infrequent in Argentina (5,6) (Appendix 3). The X family has been associated with high transmissibility (7,8), and SIT119 could have been imported from Brazil, considering the frequent cross-border movements to and from Chaco (Appendix 3). Further phylogenomic studies are warranted to determine the precise origin of that MDR strain.
Several factors converged in the outbreak. It started as intrahospital transmission to a healthcare worker, who spread the disease to her cohabitants (Figure 2). Despite her background, the family was poorly receptive to and not compliant with treatment. On the other hand, some healthcare workers were not appropriately prepared to manage MDR TB. Delayed diagnosis, poor compliance, and administration of suboptimal regimens led to long periods of culture positivity, amplification of resistance, and an alarmingly high mortality rate (53%). In addition to lack of effective drugs, host and bacterial genetic factors could have played a role. Several patients were relatives, which suggests genetic susceptibility to TB. Conversely, the observed mortality rate suggests higher virulence of the Ch strain. Although challenging to assess their relative effect, those biological and societal factors collectively shaped the outbreak outcome.
We gained valuable insights from our study. The phylogenetic analysis strongly suggests additional missing cases, and although no new cases were diagnosed, MDR TB surveillance in Chaco must be strengthened. Of note, Ch genotype can be suspected by detecting the rpoB double mutation through GeneXpert and other molecular tests (data not shown). Next-generation tools, including novel drugs and WGS, are available, but clinical suspicion of MDR-TB remains crucial for their effective use. Continuing education and active engagement of healthcare professionals and the community are vital for managing future outbreaks.
Mrs. Paul is a professional of the Servicio de Micobacterias, INEI, ANLIS Dr. “C. G. Malbrán” and the Hospital Piñero, Buenos Aires, Argentina, with a research interest in the microbiological diagnosis of mycobacterial diseases.
Acknowledgments
We thank Susana Imaz for the helpful discussion.
This work was supported by PICT-2021-I-GRF1 TI-00049 of the Agencia I+D+i, Argentina. The funder had no role in study design. The authors have no relevant financial or nonfinancial interests to disclose.
Raw sequences were deposited in the European Nucleotide Archive. Accession numbers are available in Appendix 1.
References
- Argentina Ministerio de Salud. Boletín N° 7 tuberculosis y lepra en la argentina coordinación de tuberculosis y lepra [cited 2024 Nov 30]. https://www.argentina.gob.ar/sites/default/files/2024/04/boletin_tuberculosis_2024_1642024.pdf
- Ritacco V, López B, Ambroggi M, Palmero D, Salvadores B, Gravina E, et al.; National TB Laboratory Network. HIV infection and geographically bound transmission of drug-resistant tuberculosis, Argentina. Emerg Infect Dis. 2012;18:1802–10. DOIPubMedGoogle Scholar
- World Health Organization. Catalogue of mutations in Mycobacterium tuberculosis complex and their association with drug resistance, 2nd ed. [cited 2024 Nov 30]. https://www.who.int/publications/i/item/9789240082410
- Gagneux S, Long CD, Small PM, Van T, Schoolnik GK, Bohannan BJM. The competitive cost of antibiotic resistance in Mycobacterium tuberculosis. Science. 2006;312:1944–6. DOIPubMedGoogle Scholar
- Yokobori N, Paul R. Informe técnico sobre la tuberculosis multidrogorresistente en la Argentina, 2023 [cited 2024 Nov 30]. https://sgc.anlis.gob.ar/handle/123456789/2618
- Monteserin J, Paul R, Gravina E, Reniero A, Hernandez T, Mazzeo E, et al. Genotypic diversity of Mycobacterium tuberculosis in Buenos Aires, Argentina. Infect Genet Evol. 2018;62:1–7. DOIPubMedGoogle Scholar
- Comín J, Cebollada A, Ibarz D, Viñuelas J, Vitoria MA, Iglesias MJ, et al. A whole-genome sequencing study of an X-family tuberculosis outbreak focus on transmission chain along 25 years. Tuberculosis (Edinb). 2021;126:
102022 . DOIPubMedGoogle Scholar - Bishai WR, Dannenberg AM Jr, Parrish N, Ruiz R, Chen P, Zook BC, et al. Virulence of Mycobacterium tuberculosis CDC1551 and H37Rv in rabbits evaluated by Lurie’s pulmonary tubercle count method. Infect Immun. 1999;67:4931–4. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: February 21, 2025
1These first authors contributed equally to this article.
Table of Contents – Volume 31, Number 3—March 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Noemí Kaoru Yokobori, Servicio de Micobacterias, Departamento de Bacteriología, INEI, ANLIS “Dr. C. G. Malbrán.” Vélez Sarsfield 563, Ciudad Autónoma de Buenos Aires, C1282AFF, Argentina
Top