Volume 32, Number 1—January 2026
Research
Clinical Manifestations of Emerging Trichosporon spp. Infections, France
Cite This Article
Citation for Media
Abstract
Fungi in the family Trichosporonaceae are rarely involved in invasive disease but are frequently associated with colonization or respiratory allergic infection. Trichosporonaceae exhibit intrinsic resistance to echinocandin antimicrobial drugs, posing challenges for treatment and contributing to high mortality rates. We complied a nationwide analysis of 112 cases of invasive disease caused by Trichosporon spp. and related fungi, diagnosed in France over 20 years, that combined clinical data, susceptibility profiles, and molecular identification. We identified 12 species; T. asahii was the most common species recovered, and the new species T. austroamericanum was next. Comparison of clinical data highlighted species and genotypic differences, such as a much higher proportion of children infected by T. asahii and major differences in antimicrobial drug susceptibility. Correct identification is not only of epidemiologic interest but also necessary for patient management because of the varying clinical and microbiological characteristics found in different species.
Among the wide range of fungi responsible for invasive infections in humans, species within the Trichosporonaceae family are generally considered rare or uncommon pathogens (1–4). However, recent reports indicate an increasing incidence in both high-income and resource-limited countries over the past decade (2,4–6).
Trichosporonaceae is a family of basidiomycetous, yeast-like fungi that produce arthroconidia and are commonly found in air, soil, and water worldwide (7). Trichosporonaceae can also be recovered from contaminated materials or medical devices. Some species are part of the normal or transient human microbiota, particularly on the skin and in the gastrointestinal tract (8–11). After taxonomic revisions, clinically relevant Trichosporonaceae are now distributed into 3 genera, Trichosporon, Apiotrichum, and Cutaneotrichosporon. Each genus contains multiple species known to cause invasive infections in humans (12–14). T. asahii remains the most frequently reported species responsible for invasive fungal disease (IFD) caused by Trichosporonaceae (5,6,9,15–17), but it is also known to cause summer-type hypersensitivity pneumonitis, particularly in Japan (18,19). This species is also considered the most virulent among Trichosporonaceae and demonstrates higher MICs for amphotericin B and azoles than other fungi (15,17,20–22). The distribution of other species varies, but typically Cutaneotrichosporon dermatis, T. asteroides, C. mucoides, T. inkin, and T. faecale are relatively commonly involved in IFD (2,4,5,17,21,23,24), and T. inkin is recognized as a leading cause of white piedra (25).
IFD caused by Trichosporonaceae has a high mortality rate, ranging from 30% to 90% (4,24,26,27). Such infections are commonly associated with hematologic malignancies (1,2,28) and are frequently reported in pediatric populations (26). Immunosuppressed patients are particularly at risk, especially those with central venous catheters, urinary or peritoneal catheters, broad-spectrum antimicrobial drug use, corticosteroid therapy, intensive care unit (ICU) stays, or prior exposure to echinocandins such as caspofungin, to which Trichosporonaceae fungi are intrinsically resistant (1,3,4,23,29,30). Clusters of infection have been described previously (16). Current treatment guidelines recommend voriconazole monotherapy for IFD caused by Trichosporonaceae (28,31), although other azoles and amphotericin B are also commonly used. Some studies advocate combination therapy with amphotericin B and voriconazole (17,20).
Despite the clinical relevance of Trichosporonaceae infections, epidemiologic data from multicentric studies remain scarce (4), and most information stems from case reports or small patient cohorts (6,27). Because of the variability in antimicrobial drug susceptibility across species, accurate identification is essential for both epidemiologic understanding and clinical management (1,21). In this article, we report 112 episodes of IFD caused by Trichosporonaceae, diagnosed during 2002–2022 in France. The cases were documented across 41 centers and are supported by clinical data, precise molecular identification, and antimicrobial susceptibility testing.
Clinical Data
We included in the study all first episodes of IFD caused by Trichosporonaceae notified at the National Reference Center for Invasive Mycoses and Antifungals (NRCMA) during 2002–2022. Demographic and clinical data concerning the patients were collected during prospective national surveillance programs. The surveillance of the NRCMA was approved by the Institut Pasteur Institutional Review Board 1 (approval no. 2009–34/IRB) and the Commission National de l’Informatique et des Libertés, according to French regulations. The YEASTS program collected information and strains corresponding to fungemia episodes in hospitals near Paris during 2002–2022 (1). The Réseau de Surveillance des Infections Fongiques (RESSIF) program centralized data on IFD episodes, without selection bias, from 36 hospitals throughout France, diagnosed during 2012 and 2022 (32).
We collected demographic and clinical data by using electronic case report form designed on the VOOZANOO platform (http://www2.voozanoo.net). We conducted statistical analyses by using Stata software version 17 (StataCorp, LLC, https://www.stata.com). We expressed categorical variables as percentages and continuous variables as medians +SD. We evaluated differences between the groups by using χ2 or Fisher exact tests and considered p values <0.05 statistically significant. We conducted Shapiro-Wilk tests to determine the distribution of MIC values for genotypes 1, 3, and 4 of T. asahii and then performed a Kruskal Wallis or analysis of variance test.
Isolates
As part of this prospective surveillance program, clinical isolates were sent to the NRCMA for complementary investigations, including species identification and in vitro antifungal susceptibility testing by the EUCAST method. Depending on the period, methods for identification were different (ID32C carbon assimilation profiles or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry profiles associated with internal transcribed spacer [ITS] or intergenic spacer [IGS] region sequencing), but when it was possible ITS+IGS regions were sequenced prospectively or retrospectively. For the isolates (n = 3) not sent to the active surveillances programs YEASTS or RESSIF (32,33) and from before 2008, retrospective identification was not possible.
We amplified ITS regions by PCR by using panfungal primers V9D (5′-TTAAGTCCCTGCCCTTTGTA-3′) (34) and LS266 (5′-GCATTCCCAAACAACTCGACTC-3′) (35) and the IGS region by using 26SF and 5SR, as previously reported (14). We edited sequences by using Geneious Prime software (https://www.geneious.com). We trimmed ITS region sequences with sequences of primers ITS1 (5′-TCCGTAGGTGAACCTGCGG-3′) and ITS4 (5′-GCATATCAATAAGCGGAGGA-3′) and IGS1 region sequences by using sequences SCTTTGSACT and ACYGCATCC, adapted from previous reports (14).
For species identification, we compared concatenated sequences of ITS and IGS regions of the clinical isolates with concatenated sequences of type strains. When sequences of isolates had a percentage of similarity with sequence of type strain >98%, we considered isolates as belonging to the same species. When the percentage was 90%–98%, we suggested that isolates could belong to a putative undescribed species, and we named them with a cf. in front of the species name. For those isolates, we deposited sequences into GenBank (accession nos. PV575975–8).
We conducted multiple alignments of 106 ITS+IGS concatenated sequences of 1,556 bp (95 clinical isolates and 11 type strains) by using multiple sequence comparison by log-expectation alignment and constructed a neighbor-joining tree by using a Hasegawa-Kishino-Yano model with a bootstrap analysis of 1,000 replicates. We used a newick tree to design a cladogram with Itol software version 1.9 (https://itol.embl.de). We used IGS1 sequences for T. asahii isolates to determine genotype.
Antimicrobial Susceptibility Profile
We determined MICs for fluconazole, voriconazole, posaconazole, and flucytosine for all isolates according to the EUCAST broth microdilution standardized method (https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Files/EUCAST_E.Def_7.4_Yeast_definitive_revised_2023.pdf). We also determined caspofungin, micafungin, and amphotericin B MICs with a modified version of the protocol, which uses AM3 medium instead of RPMI medium as described previously (36).
We calculated values of MIC inhibiting at least 50% (MIC50) or 90% (MIC90) of the isolates among 1 species. Of note, neither EUCAST nor Clinical and Laboratory Standards Institute currently publish breakpoints for any Trichosporonacea species. Recently, EUCAST proposed interpretation of amphotericin B and anidulafungin MICs for Trichosporon spp.; but because we did not use standard conditions to determine MICs for amphotericin B, we cannot take those values into account. However, epidemiologic cutoffs have been proposed for fluconazole for T. asahii and for fluconazole and voriconazole for C. dermatis (https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Files/EUCAST_guidance_for_Rare_yeast_with_no_breakpoints_final_clean_19-06-2024.pdf).
Phenotypic Observation
We examined the macroscopic appearance of 10 isolates belonging to species of the ovoides clade, containing the main Trichosporon species involved in IFD. Those isolates were CBS 4828 type of T. faecale, CNRMA15.795 T. cf. faecale, CBS 5585 neotype of T. inkin, CNRMA20.443 T. austroamericanum, CBS 2482 type of T. coremiiforme, CNRMA19.523 T. cf. coremiiforme, CBS 7556 neotype of T. ovoides, CBS 9051 type of T. lactis, CBS 9052 type of T. caseorum, and CBS 2479 type of T. asahii.
We prepared a suspension concentrated at 2.105 cells/mL on the basis of a fresh culture of isolates in sterile water. We determined concentration by using luna cell counting slides (Logos Biosystems Inc., https://logosbio.com). Then, we deposited 2 µL of the solution on Sabouraud agar plates and incubated at 20°C. We measured the size of the colony after 4, 5, 6, 7, and 10 days and noted color and appearance.
Episode Characteristics
During 2002–2022, a total of 112 cases of IFD caused by Trichosporonaceae, mainly bloodstream infection (77.7%), concerning 112 patients, were reported to the NRCMA from 41 hospitals in France (37 metropolitan and 4 overseas) (Table 1). Most patients were male (66.1% vs. 33.9% female); median age was 43.77 years, and a high percentage were extreme ages (18.8% children <15 years of age and 17.9% adults >65 years of age). The main underlying conditions were hematologic malignancies (39.3%), recent surgery (<30 days from diagnosis; 28.6%), and solid organ transplantation (11.6%). Twelve patients also had diabetes mellitus, 7 had traumas (generally serious accidents involving contact with plants, such as being crushed by a tree, or mower or rototiller accidents resulting in multiple fractures or amputations), and 23 were neutropenic. Risk factors associated were stay in ICU (45.9%), presence of catheter (56.3%), immunosuppressive drugs (37.5%), or administration of steroids (22.3%). At least 33.9% of patients received antimicrobial drugs before IFD diagnosis, mainly echinocandins (24.1%). Most patients received antimicrobial drugs after diagnosis (90.2%), mainly with voriconazole (57.1%). Mortality by day 30 after diagnosis was 38.4%.
Of note, among the 112 episodes, 14 corresponded to mixed infections. Those patients were simultaneously infected with 1 or 2 additional fungal species, mainly ascomycetous yeast (n = 9) at the same infection site (Appendix Table). Those episodes were caused by 6 different species of Trichosporonaceae, although T. asahii was involved in most cases (9/14).
Species Diversity
Figure 1

Figure 1. Cladogram of 94 clinical isolates and 11 reference strains from study of clinical manifestations of emerging Trichosporonspecies infections, France, 2002–2022. Tree was designed using Itol software version 1.9...
Among the 112 episodes studied, 101 isolates from 101 episodes were sent to the NRCMA. On the basis of the ITS+IGS sequencing, 94 isolates belonged to 9 already described species, distributed across 3 genera (Trichosporon [n = 5], Apiotrichum [n = 2], Cutaneotrichosporon [n = 2]). Seven isolates corresponded to 3 putative unknown species: 4 closely related to T. faecale (GenBank accession nos. PV575976 and PV575977), 2 to T. coremiiforme (GenBank accession no. PV575975) and 1 to A. loubierii (GenBank accession no, PV575978) (Figure 1).
Figure 2

Figure 2. Proportions of species involved in invasive trichosporonosis cases from study of clinical manifestations of emerging Trichosporon species infections, France, 2002–2022. The cf. designation indicates putative undescribed species....
Most isolates belonged to the Trichosporon genus (90.1%). Two species represented most cases of IFD caused by Trichosporonaceae in France: T. asahii (51.5%) and the species recently described as T. austroamericanum (22.8%), which is closely related to T. inkin (Figure 2). Among the 58 cases of T. asahii, 51 isolates were received at the NRCMA. On the basis of IGS sequencing, 6 genotypes were identified, mainly genotype 1 (n = 25) and genotypes 3 (n = 11) and 4 (n = 11), followed by genotype 7 (n = 2), genotype 5 (n = 1), and 1 isolate with an undefined allele.
Figure 3
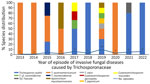
Figure 3. Species distribution over time for RESSIF survey used in a study of the clinical manifestations of emerging Trichosporonspecies infections, France, 2002–2022. Number of episodes diagnosed in the centers...
Episodes of IFD caused by Trichosporonaceae were reported under several national surveillance programs. If we compare the distribution of species and the number of episodes by year over the same period for the RESSIF program and the YEASTS program, the proportion of T. asahii is higher among the YEASTS program than among the RESSIF survey but the opposite for T. austroamericanum. A trend for an increased number of episodes over time in the RESSIF survey was seen (Figure 3).
In Vitro Antimicrobial Drug Susceptibility
Figure 4

Figure 4. Voriconazole MIC distribution for 3 species of Trichosporon from study of clinical manifestations of emerging Trichosporon species infections, France, 2002–2022. MICs determined by using the EUCAST method....
Voriconazole appears to be the most active antifungal agent in vitro (Table 2), with the lowest MIC50 or MIC90 values and ranges of MICs for all species, except for A. mycotoxinivorans, for which both isolates have lower values for posaconazole than voriconazole. Conversely, all isolates of all species have high MICs to flucytosine (>4 mg/L and all MIC50 determined ≥32 mg/L) and to echinocandins (data not shown). Trichosporon asahii, A. loubieri, A. mycotoxinivorans, and isolates closely related to T. faecale have reduced susceptibility to amphotericin B compared with other Trichosporonaceae species. More precisely, T. asahii isolates belonging to genotype 4 tend toward lower MIC50 or MIC90 values for azoles and amphotericin B than isolates of genotypes 1 and 3 (genotype 1 displayed the highest MIC50 or MIC90 for all antimicrobial drugs), but the differences were statistically significant only for amphotericin B (p = 0.0073). EUCAST recently defined epidemiologic cutoff values for fluconazole (wild-type <16 mg/L) for T. asahii and for fluconazole (wild-type <16 mg/L) and voriconazole (wild-type <0.125 mg/L) for C. dermatis. Taking those values into account, we can see only 4 isolates of genotype 1 can be considered resistant to fluconazole. We found no resistant isolates among the other genotypes or for C. dermatis strains. Furthermore, T. asahii have higher MICs for azoles and amphotericin B than T. austroamericanum and T. inkin with a difference in voriconazole MIC distribution (Figure 4).
Growth Rate and Morphologic Aspect
Figure 5

Figure 5. Macroscopic aspect of colonies grown on Sabouraud agar plates incubated 10 days at 20°C for 10 isolates recovered from study of clinical manifestations of emerging Trichosporonspecies infections, France,...
On the basis of the growth rate measured for 10 isolates belonging to different species of Trichosporon (Appendix Figure), we observed that T. coremiiforme and isolates corresponding to the potential T. cf. coremiiforme (isolate name CNRMA19.523) species had the highest growth rate, whereas T. inkin and T. austroamericanum had reduced but similar growth rate. All isolates grew as white colonies on Sabouraud agar plate and were generally creamy, although some species appeared smooth or flat to domed and wrinkled (Figure 5).
T. asahii versus T. austroamericanum
Episodes involving only 1 species (excluding mixed infections) and those with isolates sent to NRCMA were included in this comparison, which corresponds to 44 episodes of T. asahii infection and 22 of T. austroamericanum. A higher proportion of women and children among the patients infected with T. asahii were observed, whereas the proportion of men was much higher among patients infected with T. austroamericanum. Furthermore, infections because of T. austroamericanum were more frequently associated with recent surgery (p = 0.03) or solid organ transplantation (p = 0.008) (Table 3).
In this report, we describe demographic, clinical, and molecular characteristics of a large collection of 112 cases of IFD caused by Trichosporonaceae fungi diagnosed in France throughout 2 decades during multicentric national prospective surveillance programs. As mentioned in other studies, we observed a high proportion of children among the patients (18.8%) but with a significant difference in proportion depending on the species (26). As outlined in this study, most cases of IFD caused by Trichosporonaceae are bloodstream infections (77.7%) and occur in patients with underlying conditions such as hematologic malignancy (39.3%), recent surgery (28.6%), or solid organ transplant (11.6%) (1,2,28). A recent study concluded that, in cases of fungemia caused by Trichosporon spp., advanced age, use of mechanical ventilation, and persistent neutropenia were associated with poor prognosis (4). Another study demonstrated that exposure to caspofungin is a risk factor associated with fungemia caused by Trichosporon spp. (1). Similarly, the risk factors that we found frequently were hospitalization in ICU (45.9%), presence of catheter (56.3%), and exposure to antimicrobial drugs (33.9%), primarily echinocandins (27/38).
On the basis of the data from RESSIF, we seem to be observing a trend in France toward an increase in the number of cases of IFD caused by Trichosporonaceae. However, the incidence of those infections is difficult to determine precisely, because some participating centers did not participate exhaustively over the entire study period.
Sequencing of ITS+IGS regions of rDNA enabled us to identify >12 different species of Trichosporonaceae responsible for 112 IFD cases in 41 different hospitals in France during 2002–2022. Of note, all cases reported from overseas territories were because of T. asahii only. We suggest that 7 cases were because of putative undescribed species, for which additional molecular characterizations such as whole-genome sequencing analysis are now warranted. As expected, most cases were caused by T. asahii, but unexpectedly, the recently described species T. austroamericanum ranked second (12). The percentage of children was significantly lower among patients infected with this new species (4.5%) than among those infected with T. asahii (29.5%; p = 0.024). On the other hand, the percentage of men was much higher (86% vs. 52%; p = 0.007). In addition, T. asahii was more frequently involved in bloodstream infections or exposure to an antimicrobial drug, whereas T. austroamericanum was more frequently associated with recent surgery (p = 0.03) and solid organ transplant (p = 0.008) (Table 3).
Sequencing of the IGS region for T. asahii isolates is described as a useful tool for genotyping this species. At least 13 different genotypes have already been identified, some of which appear to have geographic preferences. Genotypes 1, 3, and 4 seem to be more frequent worldwide (5,15,16,23,37). Among the 101 isolates received at the NRCMA during the study period we report, the 51 isolates of T. asahii belonged to 6 different genotypes, and we confirmed the major genotype was 1 (49%), followed by genotypes 3 (21%) and 4 (21%). Of note, genotype 3 is frequently reported in the United States, in Thailand, and in the houses of summer-type hypersensitivity pneumonitis patients in Japan (14,17). Of interest, among the 11 patients infected with genotype 3 in this study, at least 6 were recovered from patients born or diagnosed in the Americas. Surprisingly, according to the genotype and excluding cases of mixed infections, 13 of 21 patients infected by genotype 1 died within 30 days of diagnosis: 5 of 11 for genotype 3 and only 1 of 8 for genotype 4. Those results could suggest some epidemiologic characteristic related to genotype or some difference in terms of virulence.
We confirmed that no matter the species or genotypes, voriconazole is the most effective antimicrobial drug in vitro against isolates belonging to the Trichosporonaceae family (17,20). Because of the small number of isolates for 10 species, we can only give the MIC values obtained for informational purposes. However, there are some differences worth noting: T. asahii, A. loubieri, A. mycotoxinivorans, and the isolates closely related to T. faecale have a lower susceptibility to amphotericin B compared with other species. Furthermore, T. asahii has higher MICs for azoles and amphotericin B than do T. austroamericanum and T. inkin. Some differences are noticed between genotypes; genotype 1 has the highest MIC for all antimicrobial drugs tested, whereas genotype 4 has lower MICs to azoles and amphotericin B than isolates of genotypes 1 and 3. Some studies reported a lower susceptibility for certain genotypes (17,37,38) and one study found that genotype 7 isolates have the highest MIC90 values for azoles, suggesting those isolates contributed to the increasing rates of voriconazole non-wild–type isolates observed in the past 10 years (37). In this study, the proportion of genotype 7 was too small to calculate MIC90s. Nevertheless, determining natural diversity would be useful to explain differences in susceptibility or even virulence, possibly linked to environmental pressures such as repeated exposure to azoles, because that mechanism is known in other pathogenic fungi (39–41).
We confirmed that T. asahii, especially genotype 1, is the major species of the Trichosporonaceae family involved in human IFD. We also confirmed that the pediatric population is at a higher risk and that the most frequent underlying conditions associated with infection are hematologic malignancies, recent surgery, and solid organ transplantation. We identified 3 main genotypes recovered among the patients diagnosed in French hospitals (genotypes 1, 3, and 4). Of note, we observed that genotype 4 seems to be more frequently associated with trauma and having lower MICs values for amphotericin B and azoles, compared with other genotypes. Species and genotype identification of environmental isolates will be necessary to increase the knowledge about natural reservoirs, diversity, and virulence.
We observed that the recently described T. austroamericanum, closely related to T. inkin and frequently misidentified by using carbon profile assimilation pattern, 26S, ITS sequencing, or matrix-assisted laser desorption/ionization time-of-flight mass spectrometry, was the second most common Trichosporonaceae family involved in human IFD. When compared with the clinical data of patients infected with T. asahii, we found very different species characteristics. In contrast, T. inkin, T. faecale, and C. dermatis, which are frequently identified as responsible for non–T. asahii IFD, were rarely involved in our survey (4,17,21).
In conclusion, this study confirms that the correct identification of Trichosporonaceae species and genotypes is not only of epidemiologic interest but also critical for patient management. Certain clinical and microbiological characteristics, such as in vitro susceptibility to antimicrobial agents, can vary according to species. Clinicians must have the correct organism identification to treat patients correctly.
Dr. Desnos-Ollivier is a deputy director of the French National Reference Center for invasive Mycoses and Antifungals at the Institut Pasteur, Paris, France. She is involved in managing the national surveillance program of invasive fungal infections in yeast identification, the study of antifungal resistance, cluster cases, and the emergence of new yeast species.
Acknowledgment
Funding was provided by Santé Publique France.
References
- Bretagne S, Renaudat C, Desnos-Ollivier M, Sitbon K, Lortholary O, Dromer F; French Mycosis Study Group. Predisposing factors and outcome of uncommon yeast species-related fungaemia based on an exhaustive surveillance programme (2002-14). J Antimicrob Chemother. 2017;72:1784–93. DOIPubMedGoogle Scholar
- Colombo AL, Padovan AC, Chaves GM. Current knowledge of Trichosporon spp. and Trichosporonosis. Clin Microbiol Rev. 2011;24:682–700. DOIPubMedGoogle Scholar
- Lima YP, Dias VC. Trichosporon spp.: what’s new? Future Microbiol. 2024;19:373–5. DOIPubMedGoogle Scholar
- Nobrega de Almeida J, Francisco EC, Holguín Ruiz A, Cuéllar LE, Rodrigues Aquino V, Verena Mendes A, et al. Epidemiology, clinical aspects, outcomes and prognostic factors associated with Trichosporon fungaemia: results of an international multicentre study carried out at 23 medical centres. J Antimicrob Chemother. 2021;76:1907–15. DOIPubMedGoogle Scholar
- Kuo SH, Lu PL, Chen YC, Ho MW, Lee CH, Chou CH, et al. The epidemiology, genotypes, antifungal susceptibility of Trichosporon species, and the impact of voriconazole on Trichosporon fungemia patients. J Formos Med Assoc. 2021;120:1686–94. DOIPubMedGoogle Scholar
- Liao Y, Lu X, Yang S, Luo Y, Chen Q, Yang R. Epidemiology and outcome of Trichosporon fungemia: a review of 185 reported cases from 1975 to 2014. Open Forum Infect Dis. 2015;2:ofv141. DOIGoogle Scholar
- Sugita T, Nishikawa A, Ichikawa T, Ikeda R, Shinoda T. Isolation of Trichosporon asahii from environmental materials. Med Mycol. 2000;38:27–30. DOIPubMedGoogle Scholar
- Cho O, Matsukura M, Sugita T. Molecular evidence that the opportunistic fungal pathogen Trichosporon asahii is part of the normal fungal microbiota of the human gut based on rRNA genotyping. Int J Infect Dis. 2015;39:87–8. DOIPubMedGoogle Scholar
- Li H, Guo M, Wang C, Li Y, Fernandez AM, Ferraro TN, et al. Epidemiological study of Trichosporon asahii infections over the past 23 years. Epidemiol Infect. 2020;148:
e169 . DOIPubMedGoogle Scholar - Mehta V, Nayyar C, Gulati N, Singla N, Rai S, Chandar J. A comprehensive review of Trichosporon spp.: an invasive and emerging fungus. Cureus. 2021;13:
e17345 . DOIPubMedGoogle Scholar - Zhang E, Sugita T, Tsuboi R, Yamazaki T, Makimura K. The opportunistic yeast pathogen Trichosporon asahii colonizes the skin of healthy individuals: analysis of 380 healthy individuals by age and gender using a nested polymerase chain reaction assay. Microbiol Immunol. 2011;55:483–8. DOIPubMedGoogle Scholar
- Francisco EC, Desnos-Ollivier M, Dieleman C, Boekhout T, Santos DWCL, Medina-Pestana JO, et al. Unveiling Trichosporon austroamericanum sp. nov.: a novel emerging opportunistic basidiomycetous yeast species. Mycopathologia. 2024;189:43. DOIPubMedGoogle Scholar
- Liu XZ, Wang QM, Göker M, Groenewald M, Kachalkin AV, Lumbsch HT, et al. Towards an integrated phylogenetic classification of the Tremellomycetes. Stud Mycol. 2015;81:85–147. DOIPubMedGoogle Scholar
- Sugita T, Nakajima M, Ikeda R, Matsushima T, Shinoda T. Sequence analysis of the ribosomal DNA intergenic spacer 1 regions of Trichosporon species. J Clin Microbiol. 2002;40:1826–30. DOIPubMedGoogle Scholar
- Arabatzis M, Abel P, Kanellopoulou M, Adamou D, Alexandrou-Athanasoulis H, Stathi A, et al. Sequence-based identification, genotyping and EUCAST antifungal susceptibilities of Trichosporon clinical isolates from Greece. Clin Microbiol Infect. 2014;20:777–83. DOIPubMedGoogle Scholar
- Desnos-Ollivier M, Maufrais C, Pihet M, Aznar C, Dromer F; French Mycoses Study Group. Epidemiological investigation for grouped cases of Trichosporon asahii using whole genome and IGS1 sequencing. Mycoses. 2020;63:942–51. DOIPubMedGoogle Scholar
- Guo LN, Yu SY, Hsueh PR, Al-Hatmi AMS, Meis JF, Hagen F, et al. Invasive infections due to Trichosporon: species distribution, genotyping, and antifungal susceptibilities from a multicenter study in China. J Clin Microbiol. 2019;57:e01505–18. DOIPubMedGoogle Scholar
- Nakajima A, Saraya T, Mori T, Ikeda R, Sugita T, Watanabe T, et al. Familial summer-type hypersensitivity pneumonitis in Japan: two case reports and review of the literature. BMC Res Notes. 2013;6:371. DOIPubMedGoogle Scholar
- Sugita T, Ikeda R, Nishikawa A. Analysis of Trichosporon isolates obtained from the houses of patients with summer-type hypersensitivity pneumonitis. J Clin Microbiol. 2004;42:5467–71. DOIPubMedGoogle Scholar
- Desnos-Ollivier M, Lortholary O, Bretagne S, Dromer F. Azole susceptibility profiles of more than 9,000 clinical yeast isolates belonging to 40 common and rare species. Antimicrob Agents Chemother. 2021;65:e02615–20. DOIPubMedGoogle Scholar
- Francisco EC, de Almeida Junior JN, de Queiroz Telles F, Aquino VR, Mendes AVA, de Andrade Barberino MGM, et al. Species distribution and antifungal susceptibility of 358 Trichosporon clinical isolates collected in 24 medical centres. Clin Microbiol Infect. 2019;25:909.e1–5. DOIPubMedGoogle Scholar
- Kurakado S, Miyashita T, Chiba R, Sato C, Matsumoto Y, Sugita T. Role of arthroconidia in biofilm formation by Trichosporon asahii. Mycoses. 2021;64:42–7. DOIPubMedGoogle Scholar
- Parashar A, Rastogi V, Prakash H, Pandey A, Rudramurthy SM. Intergenic spacer (IGS-1) region sequence-based identification, genotypic analysis, and antifungal susceptibility of clinical Trichosporon species. Indian J Med Microbiol. 2023;45:
100390 . DOIPubMedGoogle Scholar - Chagas-Neto TC, Chaves GM, Melo AS, Colombo AL. Bloodstream infections due to Trichosporon spp.: species distribution, Trichosporon asahii genotypes determined on the basis of ribosomal DNA intergenic spacer 1 sequencing, and antifungal susceptibility testing. J Clin Microbiol. 2009;47:1074–81. DOIPubMedGoogle Scholar
- Guerrero-Ponce AE, Araiza J, Tirado-Sánchez A, Bonifaz A. Review article white piedra: review of 131 cases. Mycoses. 2024;67:
e13668 . DOIPubMedGoogle Scholar - Akaslan Kara A, Çay Ü, Yalçınkaya R, Erdeniz EH, Tural Kara T, Özdemir H, et al. Bloodstream infections due to Trichosporon species in paediatric patients: Results from the first national study from Turkey. J Mycol Med. 2022;32:
101229 . DOIPubMedGoogle Scholar - de Almeida Júnior JN, Hennequin C. Invasive Trichosporon infection: a systematic review on a re-emerging fungal pathogen. Front Microbiol. 2016;7:1629. DOIPubMedGoogle Scholar
- Chen SC, Perfect J, Colombo AL, Cornely OA, Groll AH, Seidel D, et al. Global guideline for the diagnosis and management of rare yeast infections: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. 2021;21:e375–86. DOIPubMedGoogle Scholar
- Bayramoglu G, Sonmez M, Tosun I, Aydin K, Aydin F. Breakthrough Trichosporon asahii fungemia in neutropenic patient with acute leukemia while receiving caspofungin. Infection. 2008;36:68–70. DOIPubMedGoogle Scholar
- Cordeiro RA, Aguiar ALR, da Silva BN, Pereira LMG, Portela FVM, de Camargo ZP, et al. Trichosporon asahii and Trichosporon inkin biofilms produce antifungal-tolerant persister cells. Front Cell Infect Microbiol. 2021;11:
645812 . DOIPubMedGoogle Scholar - Arendrup MC, Boekhout T, Akova M, Meis JF, Cornely OA, Lortholary O; European Society of Clinical Microbiology and Infectious Diseases Fungal Infection Study Group; European Confederation of Medical Mycology. ESCMID and ECMM joint clinical guidelines for the diagnosis and management of rare invasive yeast infections. Clin Microbiol Infect. 2014;20(Suppl 3):76–98. DOIPubMedGoogle Scholar
- Bretagne S, Sitbon K, Desnos-Ollivier M, Garcia-Hermoso D, Letscher-Bru V, Cassaing S, et al.; French Mycoses Study Group. Active surveillance program to increase awareness on invasive fungal diseases: the French RESSIF network (2012 to 2018). mBio. 2022;13:
e0092022 . DOIPubMedGoogle Scholar - Dannaoui E, Paugam A, Develoux M, Chochillon C, Matheron J, Datry A, et al. Comparison of antifungal MICs for yeasts obtained using the EUCAST method in a reference laboratory and the Etest in nine different hospital laboratories. Clin Microbiol Infect. 2010;16:863–9. DOIPubMedGoogle Scholar
- de Hoog GS, Gerrits van den Ende AH. Molecular diagnostics of clinical strains of filamentous Basidiomycetes. Mycoses. 1998;41:183–9. DOIPubMedGoogle Scholar
- Masclaux F, Guého E, de Hoog GS, Christen R. Phylogenetic relationships of human-pathogenic Cladosporium (Xylohypha) species inferred from partial LS rRNA sequences. J Med Vet Mycol. 1995;33:327–38. DOIPubMedGoogle Scholar
- Desnos-Ollivier M, Bretagne S, Lortholary O, Dromer F; French Mycoses Study Group N. Brieu CH Aix, T. Chouaki, C. Damiani, A. Totet CHU Amiens, J. P. Bouchara, D. Chabasse, M. Pihet CHU Angers, S. Bland CH Annecy, V. Blanc CH Antibes, S. Branger CH Avignon, A. P. Bellanger, L. Millon CHU Besançon, C. Plassart CH Beauvais, I. Poilane Hôpital Jean Verdier, Bondy, I. Accoceberry, L. Delhaes, B. Couprie, F. Gabriel CH Bordeaux, J. Dunand, A. L. Roux, V. Sivadon-Tardy Hôpital Ambroise Paré, Boulogne Billancourt, F. Laurent CH, Bourg en Bresse, S. Legal, E. Moalic, G. Nevez, D. Quinio CHU Brest, M. Cariou CH Bretagne Sud, J. Bonhomme, C. Duhamel CHU, Caen, B. Podac CH, Chalon sur Saône, S. Lechatch CH, Charleville-Mézières, C. Soler Hopital d’Instruction des armées, Clamart, M. Cambon, C. Nourrisson, P. Poirier, D. Pons CHU, Clermont Ferrand, O. Augereau, I. Grawey CH, Colmar, N. Fauchet CHIC, Créteil, A. Bonnin, F. Dalle CHU, Dijon, P. Cahen, P. Honderlick CMC, Foch, N. Desbois, C. Miossec CHU, Fort de France, J. L. Hermann Hôpital Raymond Poincaré, Garches, M. Cornet, R. Grillot, B. Lebeau, D. Maubon, H. Pelloux CHU, Grenoble, M. Nicolas CHU, Guadeloupe, C. Aznar, D. Blanchet, J. F. Carod, M. Demar CHU, Guyane, A. Angoulvant Hôpital Bicêtre, le Kremlin Bicêtre, C. Ciupek CH, Le Mans, A. Gigandon Hôpital Marie Lannelongue, Le Plessis Robinson, B. Bouteille CH Limoges, E. Frealle, D. Poulain, B. Sendid CHU Lille, D. Dupont, J. Menotti, F. Persat, M.-A. Piens, M. Wallon CHU, Lyon, C. Cassagne, S. Ranque CHU, Marseille, T. Benoit-Cattin, L. Collet CH Mayotte, A. Fiacre CH Meaux, N. Bourgeois, L. Lachaud, P. Rispail, Y. Sterkers CHU, Montpellier, M. Machouart CHU, Nancy, F. Gay-Andrieu, P. Lepape, F. Morio CHU, Nantes, O. Moquet CH, Nevers, S. Lefrançois Hôpital Américain, Neuilly, M. Sasso CHU, Nimes, F. Reibel GH, Nord-Essone, M. Gari-Toussaint, L. Hasseine CHU Nice, L. Bret, D. Poisson CHR Orléans, S. Brun Hôpital Avicenne, Paris, C. Bonnal, C. Chochillon, S. Houzé Hôpital Bichat, Paris, A. Paugam Hôpital Cochin, Paris, N. Ait-Ammar, F. Botterel, R. Chouk CHU Henri Mondor, Paris, M. E. Bougnoux, E. Sitterle Hôpital Necker, Paris, A. Fekkar, R. Piarroux Hôpital Pitié Salpêtrière, Paris, J. Guitard, C. Hennequin, J.-L. Poirot Hôpital St Antoine, Paris, M. Gits-Muselli, S. Hamane, C. Lacroix Hôpital Saint Louis, Paris, S. Bonacorsi, P. Mariani Hôpital Robert Debré, Paris, D. Moissenet Hôpital Trousseau, Paris, C. Kauffmann-Lacroix, A. Minoza, E. Perraud, M. H. Rodier CHU Poitiers, G. Colonna CH, Porto Vecchio, A. Huguenin, D. Toubas CHU Reims, S. Chevrier, J. P. Gangneux, F. Robert-Gangneux, C. Guigen CHU Rennes, O. Belmonte, G. Hoarau, M. C. Jaffar Bandjee, J. Jaubert, S. Picot, N. Traversier CHU Réunion, L. Favennec, G. Gargala CHU, Rouen, N. Godineau, C. Tournus CH, St Denis, C. Mahinc, H. Raberin CHU, St Etienne, V. Letscher Bru CHU, Strasbourg, S. Cassaing CHU, Toulouse, P. Patoz CH Tourcoing, E. Bailly, J. Chandenier, G. Desoubeaux CHU Tours, F. Moreau CH Troyes, P. Munier CH Valence, E. Mazars CH Valenciennes, O. Eloy CH Versailles, E. Chachaty Institut Gustave Roussy, Villejuif. Echinocandins susceptibility patterns of 2,787 yeast isolates: importance of the thresholds for the detection of FKS mutations. Antimicrob Agents Chemother. 2022;66:
e0172521 . DOIPubMedGoogle Scholar - Francisco EC, de Almeida Junior JN, Queiroz-Telles F, Aquino VR, Mendes AVA, de Oliveira Silva M, et al. Correlation of Trichosporon asahii genotypes with anatomical sites and antifungal susceptibility profiles: data analyses from 284 isolates collected in the last 22 years across 24 medical centers. Antimicrob Agents Chemother. 2021;65:e01104–20. DOIPubMedGoogle Scholar
- Sun W, Su J, Xu S, Yan D. Trichosporon asahii causing nosocomial urinary tract infections in intensive care unit patients: genotypes, virulence factors and antifungal susceptibility testing. J Med Microbiol. 2012;61:1750–7. DOIPubMedGoogle Scholar
- Casadevall A, Kontoyiannis DP, Robert V. On the emergence of Candida auris: climate change, azoles, swamps, and birds. mBio. 2019;10:e01397–19. DOIPubMedGoogle Scholar
- Lestrade PPA, Meis JF, Melchers WJG, Verweij PE. Triazole resistance in Aspergillus fumigatus: recent insights and challenges for patient management. Clin Microbiol Infect. 2019;25:799–806. DOIPubMedGoogle Scholar
- Padovan ACB, Rocha WPDS, Toti ACM, Freitas de Jesus DF, Chaves GM, Colombo AL. Exploring the resistance mechanisms in Trichosporon asahii: Triazoles as the last defense for invasive trichosporonosis. Fungal Genet Biol. 2019;133:
103267 . DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: January 26, 2026
Table of Contents – Volume 32, Number 1—January 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Marie Desnos-Ollivier, Institut Pasteur, 28 rue du Docteur Roux, 75015 Paris, France
Top