Volume 32, Number 1—January 2026
Research
Detection of Novel Thermotolerant Tepidimonas sp. Bacteria in Human Respiratory Specimens, Hong Kong, China, 2024
Cite This Article
Citation for Media
Abstract
In patients with acute respiratory infections (ARIs), routine diagnostic tests often fail to identify the microbial cause; thus, many ARIs have undetermined etiology. We investigated potential involvement of thermotolerant bacteria in ARIs among patients in Hong Kong, China, by incubating blood agar inoculated with respiratory specimens at 50°C for 5 days. Among 7,257 specimens analyzed, 58 specimens from 57 patients grew thermotolerant bacteria not identified by other methods. We identified Tepidimonas spp. in 42 isolates, 3 of which appear to be a novel Tepidimonas species (tentatively Tepidimonas hongkongensis sp. nov). Genomic analysis revealed various virulence, resistance, and stress-related genomes in the 3 isolates. Tepidimonas spp. bacteria were predominantly isolated from patients with chronic lung disease and malignancies. We also detected T. hongkongensis in hospital water samples but at a lower percentage than in respiratory specimens, suggesting colonization potential. Clinical implications of T. hongkongensis remain unknown; continued surveillance could determine its role in ARIs.
Although routine bacterial culture and multiplex reverse transcription PCR for respiratory viruses and fastidious organisms are commonly performed in respiratory specimens from patients with acute respiratory syndrome, the distinct microbial cause remains unidentified in most patients. A study from China showed that among school-age children with acute respiratory infections (ARIs), 46.9% of viral and 30.9% of bacterial etiologies could be identified, but the other patients had ARIs of unknown etiology (1).
The routine practice of bacterial culture of expectorated sputum relies on blood and chocolate agar plates incubated at 35°C–37°C for 48 hours. Those methods could miss bacteria that grow poorly or very slowly at body temperature and might be overgrown by common oropharyngeal commensals. Although most respiratory pathogens are not thermotolerant, pathogens such as Aspergillus spp. fungi and the bacterium Mycobacterium xenopi are thermotolerant and have been described as causing respiratory infections, especially in patients with chronic lung disease (2).
We hypothesized that increasing the incubation temperature during culture can suppress normal flora and enable fastidious, thermotolerant bacteria to grow, possibly revealing novel pathogens contributing to ARIs. We investigated respiratory specimens by prolonged incubation of agar plates at high temperature, then subjected cultured bacterial isolates to matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry and partial 16S rRNA gene sequencing to determine whether thermotolerant bacteria were the cause of ARIs.
Study Design and Specimen Collection
We conducted a multicenter, retrospective study in a hospital network in Hong Kong, China, including a 1,700-bed university-affiliated teaching hospital (Queen Mary Hospital) and 3 extended care hospitals ranging in size from 270 to 530 beds. We included all respiratory specimens, including sputum and bronchoalveolar lavage fluid (BALF) samples, collected during January 19–May 19, 2024, and sent to the microbiology laboratory at Queen Mary Hospital for routine bacterial culture. This study was approved by the Institutional Review Board of the University of Hong Kong Special Administrative Region, People’s Republic of China/Hospital Authority Hong Kong Special Administrative Region, People’s Republic of China West Cluster (UW 25-135).
Routine Investigations Methodology
As part of routine screening, we performed Gram stains on all lower respiratory specimens to semiquantify the number of leukocytes and assess specimen quality. We observed Gram stains under light microscopy at ×100 magnification and graded stains on the basis of the number of leukocytes as trace (<25 cells), 2+ (25–75 cells), or 3+ (>75 cells) and epithelial cells as 1+ (<10 cells), 2+ (10–25 cells), or 3+ (>25 cells) in an average of 10 fields. We inoculated all samples on blood and chocolate agar plates for routine bacterial culture and also inoculated BALF samples on MacConkey agar plates. Plates routinely are incubated at 35°C at 5% CO2 and examined every 24 hours for 2 days. For this study, we also inoculated all respiratory tract samples on separate blood agar plates, incubated at 50°C, and examined plates every 24 hours for 5 days. We defined any colonies that grew from the blood agar plates at 50°C as thermotolerant bacteria, and subjected those to MALDI-TOF spectrometry and 16S rRNA PCR (3), when necessary, for bacterial identification. If the MALDI-TOF In Vitro Diagnostic database (Bruker, https://www.bruker.com) failed to identify bacteria, we performed subsequent Sanger sequencing.
16S rRNA, MALDI-TOF Spectrometry, and Whole-Genome Sequencing Methods
When MALDI-TOF spectrometry failed to identify bacterial isolates, we performed 16S rRNA sequencing. We used universal bacterial primers 16S-1F and 16S-2R and the QIAmp DNA Minikit (QIAGEN, https://www.qiagen.com) to extract DNA and sequenced on the 3500 Genetic Analyzer system (Thermo Fisher Scientific, https://www.thermofisher.com) (Appendix).
We considered bacteria that had suboptimal similarity percentages with existing bacteria in the BLAST (https://blast.ncbi.nlm.nih.gov) as possible novel species (4). We subjected those bacteria to whole-genome sequencing by using a dual platform of short- and long-read sequencing. For short-read sequencing, we performed DNA preparation by using the Nextera DNA Prep Kit, then sequenced on the iSeq100 (Illumina, https://www.illumina.com). For long-read sequencing, we used the Ligation Sequencing Kit for DNA preparation and MinION for sequencing (both Oxford Nanopore Technologies, https://nanoporetech.com) (Appendix).
Covariates of Interest
We retrieved data on patients who had thermotolerant bacterial species identified from electronic health records. Patient information included demographic data, underlying medical conditions, signs and symptoms, time from hospital admission to sample collection, hematologic parameters, inflammatory markers, and radiologic findings.
Statistical Analysis
We reported descriptive statistics as median and range and categorical variables as frequency and percentage. We used Fisher exact or χ2 tests for 2-group comparisons. We performed statistical analyses in SPSS Statistics 24.0 (IBM, https://www.ibm.com) and considered p<0.05 statistically significant.
During January 19–May 19, 2024, the microbiology laboratory collected 7,257 respiratory specimens, of which 6,766 were lower respiratory tract specimens: 5,922 expectorated sputum, 388 tracheal aspirates, and 456 bronchial specimens, including BALF and endobronchial biopsy specimens. The other 491 respiratory specimens were upper respiratory tract specimens: 113 nasal or nasopharyngeal swab samples, 283 oral or throat swab samples, and 95 gastric aspirates.
Among collected specimens, 66 (64 sputum and 2 throat swab) specimens from 65 patients grew thermotolerant bacteria that could not be identified by MALDI-TOF spectrometry (Table 1). Among the 66 thermotolerant bacterial specimens, we identified Tepidimonas spp. in 42 (63.6%, 0.6% of all respiratory specimens, 41 sputum and 1 throat swab) specimens from 41 patients by 16S rRNA sequencing; 37 were T. aquatica, 3 were undetermined Tepidimonas spp., 1 was T. taiwanensis, and 1 was T. fonticaldi.
Patients with Tepidimonas spp. bacterial isolates were from all age groups; 56.1% of patients were female and 43.9% were male (Table 2). The most common underlying conditions in the cohort were solid organ malignancy (41.5%), hypertension (36.6%), chronic lung disease (24.4%), and hyperlipidemia (24.4%). Among Tepidimonas spp. isolates, 58.5% were from sputum saved in the outpatient setting or collected <48 hours of hospital admission, suggesting a possible community source. Common clinical signs and symptoms included cough, fever, and shortness of breath. Some of the patients had abnormal chest radiograph findings, including consolidation or pulmonary infiltrates (26.8%), pleural effusion (19.5%), and chronic lung changes (24.4%). However, 34.1% of patients with Tepidimonas spp. isolated had unremarkable findings on chest radiographs, representing possible bacterial colonization of the respiratory tract.
Among laboratory characteristics of the 41 sputum specimens, 51.2% had trace leukocytes, and 46.3% had <10 epithelial cells per field (Table 3). In addition, 36.6% had growth of other pathogenic organisms, the most common of which were Haemophilus influenzae and Flavobacterium species.
Novel Species Identification
Our study identified 3 clinical isolates of a novel Tepidimonas sp. bacterium. Here, we report phenotypic characteristics and genomic features of those bacteria, including detection of virulence, antimicrobial resistance (AMR), and stress-related genes. To investigate potential sources of this bacterium, we also performed environmental sampling in the hospital.
Phenotypic Analysis and Biochemical Characteristics
The 3 undetermined sequences detected by 16S rRNA sequencing displayed 96.68%–97.59% sequence identity to known Tepidimonas spp. available in the BLAST database, suggesting that the taxonomic position of those isolates remained uncertain. The sequences were from 3 isolates (HKU77, HKU78, and HKU79) from 3 patients: 1 with pulmonary metastasis, 1 with community-acquired pneumonia, and 1 with underlying Graves’ disease and schizophrenia who had fever during hospitalization.
Gram stain of isolates HKU77, HKU78, and HKU79 revealed gram-negative, non–spore-forming, motile rods with occasional spherical enlargement (Appendix Figure, panel A). We observed small translucent and nonpigmented colonies with no hemolysis on blood agar after 24 hours of incubation. The size of colonies gradually increased with prolonged incubation. We noted no pigment production at 35°C or 42°C, but colonies displayed a slight brown pigmentation after prolonged incubation at 50°C. Optimal growth of those bacteria occurred at 50°C, and we noted no visible growth at 25°C (Appendix Figure, panels B–D). The 3 isolates did not grow in anaerobic conditions. Growth on chocolate agar and Haemophilus test medium at 50°C was similar to that for blood agar; we observed slower growth on Brucella agar. However, we noted no growth on buffered charcoal yeast extract agar or brain heart infusion agar supplemented with X and V factor. We observed no fluorescence under ultraviolet light (Table 4).
Biochemically, all 3 isolates were oxidase-positive and weakly catalase-positive (with 15% hydrogen peroxide) and tested negative for lipase, lecithinase, DNAase, and gelatinase at 50°C. The isolates were positive for nitrate reductase, glutamyl arylamidase, and tyrosine arylamidase and weakly positive for urease. Sugar fermentation (glucose, lactose, sucrose, citrate), indole, H2S production, and ortho-nitrophenyl-β-galactoside were all negative after incubation at 50°C. We evaluated enzymatic activity by using the VITEK AutoMicrobic GNI+ card (bioMérieux, https://www.biomerieux.com), which was positive for glutamyl arylamidase and tyrosine arylamidase, and 1 strain (HKU78) showed additional enzymatic activity of L-proline arylamidase and a positive Ellman’s test result.
The 3 isolates were susceptible to piperacillin, piperacillin/tazobactam, ceftazidime, amikacin, ciprofloxacin, tobramycin, and cefepime, according to the Clinical Laboratory Standards Institute Pseudomonas breakpoints (5). The MICs of penicillin for the 3 isolates were <0.016 μg/mL, and MICs of vancomycin were 48–64 μg/mL. Comparison with phenotypic characteristics of T. aquatica and T. taiwanensis showed that the Tepidimonas species from our 3 strains did not grow on buffered charcoal yeast extract agar, but both T. aquatica and T. taiwanensis did. Furthermore, T. taiwanensis is gelatinase- and nitrate-positive, but T. aquatica and the novel Tepidimonas species from our study are not (Table 4).
Comparative Genomic Characterizations
Figure 1

Figure 1. Circular genome map of novel thermotolerant Tepidimonas spp. bacteria detected in human respiratory specimens, Hong Kong, China, 2024. Using patient strain HKU77Tas the reference genome forming...
Figure 2
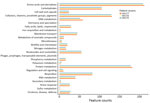
Figure 2. Comparison of feature counts of functional annotations from detection of novel thermotolerant Tepidimonasspp. bacteria in human respiratory specimens, Hong Kong, China, 2024. Annotations were determined by using Rapid...
The de novo assembly, using Illumina and Oxford Nanopore Technology reads, yielded complete genomes for the strains HKU77, HKU78, and HKU79 (Figure 1). The genome sizes of the 3 strains ranged from 2,842,968 to 2,891,522 bp, and GC content spanned 67.1%–67.2% (Table 5). We submitted the assembled genome sequences to PROKKA (https://github.com/tseemann/prokka) for annotation, which resulted in 2,695–2,786 protein-coding sequences, 3 rRNA operons, and 50–52 tRNA-coding genes (Table 5). Annotation via the RAST pipeline (Rapid Annotations using Subsystems Technology; Argonne National Laboratory, https://www.anl.gov/mcs/rast-rapid-annotation-using-subsystem-technology) indicated that the 3 strains possess a similar number of genes and subsystems, except for strain HKU78, which harbored a phage genome containing an additional integron integrase IntI1 gene related to the phages, prophages, transposable elements, and plasmids subsystem in RAST (Figure 2).
Figure 3

Figure 3. Phylogeny of novel thermotolerant Tepidimonasspp. bacteria isolated from human respiratory specimens, Hong Kong, China, 2024. Phylogenetic trees show the relationship between 3 patient strains identified in this study...
To determine the phylogenetic positions of the 3 strains within the genus Tepidimonas, we used Type (Strain) Gene Server (Leibniz Institute, https://tygs.dsmz.de) results to construct a phylogenetic tree incorporating genome data from the 3 strains and complete genomes of other Tepidimonas spp. type strains. That analysis revealed that HKU77, HKU78, and HKU79 cluster together, forming a distinct and well-supported phylogenetic clade, separate from other Tepidimonas species, and are most closely related to T. fonticaldi (Figure 3, panel A). Similarly, the phylogenetic tree constructed from core-genome sequences displayed a consistent topology (Figure 3, panel B). In silico genome-to-genome comparison demonstrated that the 3 strains from our study shared pairwise digital DNA-DNA hybridization (dDDH) values ranging from 95.3% to 97.8% among each other. Those 3 strains were most closely related to T. fonticaldi AT-A2 (dDDH value 26.1%–26.2%), followed by T. taiwanensis I1–1 (dDDH value 24.7%–24.8%), and T. charontis SPSP-6T (dDDH value 24.0%–24.3%), but the dDDH values were below the 70.0% threshold, indicating the 3 strains from our study are a different species (Table 6). On the basis of those results, we propose that strains HKU77, HKU78, and HKU79 represent a newly identified Tepidimonas species. We suggest the name Tepidimonas hongkongensis sp. nov. for the location of isolation and that strain HKU77T (GenBank accession no. CP187300) be designated as the type strain.
Virulence, AMR, and Stress-Related Genes
We characterized virulence factors of T. hongkongensis by using the Virulence Factors of Pathogenic Bacteria database (https://www.mgc.ac.cn/VFs/main.htm), on the basis of available sequences (Appendix Table 1). We identified several genes that contribute to the function of motility and adherence, some of which are similar to genes of type IV pili of Pseudomonas spp., including pilB, pilC, and pilT, contributing to the adhesion of T. hongkongensis to other cells. We also detected different genes related to immune evasion and several genes that contribute to counteracting phagocytosis in humans. Those genes included uge, which is observed to generate the capsule in Klebsiella spp. Bacteria, and algC, algU, and algW, which are responsible for alginate regulation and biosynthesis in Pseudomonas spp. bacteria. In addition, we observed genes in T. hongkongensis that are associated with secretion systems in other bacteria, including clpV (type VI secretory system), epsE, and lspG (type II secretory system). T. hongkongensis strains also contained hemE and hemL genes, which are observed in heme biosynthesis in Haemophilus spp. bacteria.
Another species, T. taiwanensis, has previously been reported to produce alkaline protease and polyhydroxyalkanoates (PHA), renewable and biodegradable polymers that can replace conventional plastic (6). Comparison of T. hongkongensis and type strain T. taiwanensis LMG22826T (GenBank accession no. CP083911) showed that T. hongkongensis contained alkaline proteases, except lysyl endopeptidase. Furthermore, T. taiwanensis possesses phaC and phaR genes that are necessary for PHA production, as well as phaZ coding PHA depolymerase. Similarly, all 3 T. hongkongensis strains possessed the phaC, phaR, and phaZ, suggesting that T. hongkongensis is associated with PHA production. Oxidation of thiosulfate to sulfate has been reported in all Tepidimonas species through the sox pathway (7), and all 3 T. hongkongensis strains contained the genes encoding the sulfur-oxidizing protein.
Using the National Center for Biotechnology Information AMRfinder (https://www.ncbi.nlm.nih.gov/pathogens/antimicrobial-resistance/AMRFinder), we found that all 3 T. hongkongensis harbored aminoglycoside resistance genes (aadA2) and a β-lactamase gene (blaOXA-2). We also identified stress-related genes, including multiple heat-shock proteins and efflux pumps, including qacL (Appendix Table 2).
Characteristics for Patients with T. hongkongensis Strains
The isolate of strain HKU77T was from a patient with pulmonary metastases. The DNA GC content was 67.2% mol; we considered this the type strain. The isolate of the second strain, HKU78, was from a patient with community-acquired pneumonia and had DNA GC content of 67.1% mol. The isolate of the third strain, HKU79, was from a patient with underlying Graves’ disease and paranoid schizophrenia and had DNA GC content of 67.2% mol.
Environmental Sample Collection and Clinical Correlations
We collected 101 water samples from the faucets in various areas of the hospital, including wards, utility rooms, bathrooms, and the pantry, after the study period in April 2025. Among collected samples, 47 (46.5%) grew thermotolerant bacteria (Table 7). From those 47 samples, we subsequently identified 43 (91.5%; 42.6% of all water samples collected) thermotolerant bacteria as Schlegelella aquatica. We identified T. hongkongensis in 2 (2.0%) water samples and Prophyrobacter cryptus bacteria in 1 (1.0%) water sample. The percentages of water samples growing S. aquatica (42.6%) and T. hongkongensis (2.0%) were higher than the rates in respiratory specimens: 0.6% S. aquatica and 0.2% T. hongkongensis (p<0.05). Although we identified >20 times more S. aquatica isolates than Tepidimonas spp. isolates in the water samples, we isolated 3 times as many Tepidimonas spp. bacteria than S. aquatica in respiratory specimens. Furthermore, among the 17 patients with Tepidimonas spp. bacteria isolated from sputum 48 hours after hospitalization (Table 2), none were hospitalized in the 2 wards from which we isolated T. hongkongensis in the water samples.
Thermotolerant bacteria can thrive under elevated temperatures, typically 45°C–60°C. Examples of thermotolerant bacteria causing human infection include Campylobacter fetus (8) and Mycobacterium xenopi (2). Various thermotolerant bacteria, such as Tepidimonas spp., have been isolated or detected in environmental hot water samples, including hot springs (9–11). However, the clinical consequences of most thermotolerant bacteria are uncertain.
In addition to Tepidimonas spp., our study identified different thermotolerant bacteria in clinical specimens, including S. aquatica, which belongs to the Comamonadaceae family and was first isolated from a hot spring in Taiwan (9) but was not known to cause human infection. In addition, we identified Vulcaniibacterium thermophilum in 4 patient samples; it was first isolated from a geothermal soil sample in Tengchong, Yunnan Province, in southwest China in 2012 (10) and was the reported cause of prosthetic joint infection in 1 case (13). In addition, Thermomonas spp. bacteria, which we detected in 2 specimens, frequently have been isolated from hot water (11,14), marine sediment (15), and soil (16–18). One study reported its detection in the naso-oropharyngeal microbiome from breast cancer patients with severe COVID-19 (19). Lactobacillus delbrueckii bacteria, which we detected in 1 specimen, commonly are used for probiotics and food fermentation (20); however, that bacterium has been reported to cause urinary tract infection and bacteremia (21–24). Finally, we detected 3 Bacillus spp. bacteria, which are known to form heat-resistant spores; although non–B. anthracis Bacillus are usually considered environmental bacteria, they can cause infection in patients with prostheses and central catheters (25,26).
The genus Tepidimonas was established in 2000 (27), and its members are gram-negative bacilli with positive catalase and oxidase activity that are motile due to a single polar flagellum. Tepidimonas spp. bacteria typically exhibit optimal growth at temperatures >45°C; therefore, most have been isolated from relatively high-temperature environments, such as hot springs and spas worldwide (9–11). As of January 25, 2026, only 8 Tepidimonas species have been validly published in the List of Prokaryotic names with Standing in Nomenclature: T. ignava, T. aquatica, T. taiwanensis, T. thermarum, T. fonticaldi, T. sediminis, T. alkaliphila, and T. charontis (https://lpsn.dsmz.de/genus/tepidimonas). Within the genus, T. taiwanensis is the only strain that uses glucose and fructose for growth, due to the presence of putative ABC glucose/mannose (gtsABCD) and fructose (frcABC) transporters (7), whereas other species are frequently referred to as asaccharolytic. Similar to a previous report (7), the novel T. hongkongensis bacterium does not use glucose and fructose for growth. Of note, T. taiwanensis produces alkaline protease and PHA, renewable and biodegradable polymers that can replace conventional plastic (6). Genome analysis revealed that T. hongkongensis contains most of the alkaline protease genes found in T. taiwanensis, as well as genes associated with PHA production (12). Analysis of stress-related genes in T. hongkongensis revealed the presence of heat-resistant protein and ATPase genes, which explain its thermotolerant characteristic.
In our study, 0.6% of respiratory specimens grew Tepidimonas spp. bacteria after prolonged incubation at 50°C, and most patients from whom specimens were collected had solid organ malignancy and chronic lung disease, although ages were wide ranging. Other Tepidimonas spp. bacteria have been detected in clinical samples. For instance, a proposed new Tepidimonas species, T. arfidensis, was cultured from a bone marrow aspirate sample from a patient with leukemia with neutropenic fever (28). Other Tepidimonas spp. bacteria have been implicated in different human microbiome studies, including the urine microbiome for urinary incontinence (29,30), the endometrial microbiome for endometriosis (31), the gut microbiome in primary sclerosing cholangitis (32), and the sinus microbiome in chronic rhinosinusitis (33). In our study, only 36.6% of the patients had growth of other pathogenic bacteria in the sputum (Table 3), suggesting that Tepidimonas spp. are pathogenic and can cause lower respiratory tract infection.
The tap water samples collected from the hospital revealed the presence of T. hongkongensis sp. nov. and a high percentage of S. aquatica. Those results align with previous findings that Tepidimonas spp. and S. aquatica bacteria are commonly found in the environment (9,34). Of note, we detected Tepidimonas spp. bacteria more frequently than S. aquatica in the water samples, but we detected more Tepidimonas spp. than S. aquatica in respiratory specimens (Tables 1, 7), suggesting that Tepidimonas spp. bacteria could have a greater potential for colonizing the human respiratory tract than other environmental bacteria.
Comparative genomic analysis revealed that all 3 T. hongkongensis strains contained various virulence genes spanning critical functional classes, including adherence, iron uptake, lipid metabolism, nutritional virulence, serum resistance, and stress adaptation, but those genes are absent in S. aquatica LMG 23380 (Appendix Table 1). Those genes support colonization of host tissue, nutrient scavenging, immune evasion, and persistence under stress, further underscoring the potential pathogenicity of T. hongkongensis. Although resistome profiling did not demonstrate substantial antimicrobial resistance in T. hongkongensis (Appendix Table 2), we did detect it in environmental samples, and its ability to acquire other resistance, such as colistin resistance, through horizontal gene transfer from other gram-negative bacteria, is not known (35,36). Therefore, further surveillance is warranted.
Whether detection of T. hongkongensis in the hospital water systems warrants interventions requires further risk assessments and studies. First, the infectious threshold of T. hongkongensis should be established to assess the risk that patients could acquire it from the water system. Furthermore, whether usual water disinfection protocols, such as chlorine or ultraviolet light, are effective against this bacterium is unknown. Ongoing vigilance and documentation will help define the baseline incidence and clinical significance for this bacterium and guide future recommendations.
The first limitation of our study is that it was conducted in a hospital network in Hong Kong; whether similar observations occur in other hospitals and countries requires further investigation. Second, we only used 50°C for agar incubation to isolate thermotolerant bacteria, which might have failed to recover other clinically relevant pathogens that do not grow at such high temperatures. Third, although isolation of Tepidimonas spp. bacteria from the clinical specimens in our study might be related to a hot water source, other studies have isolated various Tepidimonas spp. bacteria in sterile clinical specimens, suggesting this genus might not solely be an environmental contaminant. Finally, isolation of Tepidimonas spp. and other thermotolerant bacteria in respiratory specimens could represent colonization instead of respiratory pathogens. However, many patients in our study had underlying solid organ malignancy, suggesting pathogenicity is still possible in severely immunocompromised patients, such as bone marrow transplant recipients. Further studies are required to investigate the pathogenic potential of T. hongkongensis and the range of illnesses the bacteria can cause.
In conclusion, we successfully isolated 42 thermotolerant Tepidimonas spp. bacterial strains from clinical specimens, including 3 novel strains confirmed by whole-genome sequencing. We propose the name T. hongkongensis sp. nov. to describe the 3 novel strains and designation of HKU77T as the type strain of this novel species. The combination of high incubation temperature for selection, prolonged incubation for growth, and MALDI-TOF mass spectrometery and 16S rRNA sequencing enabled discovery of this novel species. Analysis of water samples from the hospital further confirmed the presence of T. hongkongensis in the environment. Although clinical implications of T. hongkongensis, especially in immunocompromised patients, are not yet known, its potential spread in water systems is concerning. Ongoing vigilance and documentation will help define the baseline incidence and clinical significance of T. hongkongensis and guide future recommendations.
Dr. Chiu is an associate consultant in the Department of Microbiology, Queen Mary Hospital, Hong Kong, China. His research interests are emerging infectious diseases and antimicrobial stewardship.
Acknowledgments
We thank the laboratory staff for additional work in processing the respiratory specimens and water samples collected during the study period.
Whole-genome sequences for strains HKU77T (GenBank accession no. CP187300), HKU78 (GenBank accession no. CP187547), and HKU79 (GenBank accession no. CP187301) are available in National Center for Biotechnology Information BioProject database (https://www.ncbi.nlm.nih.gov/bioproject) under BioProject no. PRJNA1245643.
This study was partly supported by funding from the start-up fund for new staff at the Faculty of Dentistry, The University of Hong Kong; and donations from May Tam Mak Mei Yin, Richard Yu and Carol Yu, the Shaw Foundation Hong Kong, Michael Seak-Kan Tong, Mow Lum Yip, Lee Wan Keung Charity Foundation Limited, Providence Foundation Limited (in memory of the late Lui Hac-Minh), Hui Ming, Hui Hoy and Chow Sin Lan Charity Fund Limited, The Chen Wai Wai Vivien Foundation Limited, Chan Yin Chuen Memorial Charitable Foundation, and Marina Man-Wai Lee. The funding sources had no role in the study design, data collection, analysis, interpretation, or writing of the report.
Description of Tepidimonas hongkongensis sp. nov.: T. hongkongensis (hong-kong-en′-sis. N.L. fem. adj. hongkongensis of Hong Kong, where the type strain was isolated); cells are gram-negative, aerobic, non–spore forming motile rods. Growth is optimal at temperature 50°C, no visible growth at 25°C; positive for oxidase, nitrate reductase, glutamyl arylamidase, and tyrosine arylamidase, weakly positive for urease and catalase, and lipase, lecithinase, DNAase, gelatinase, glucose, lactose, sucrose, citrate, indole, H2S production, and ONPG were negative at 50°C. Evaluation of VITEK AMS GNI card (bioMérieux) enzymatic activity using glutamyl arylamidase and tyrosine arylamidase was positive. T. hongkongensis strain HKU78 showing additional enzymatic activity of L-proline arylamidase and a positive Ellman’s test. The type strain, HKU77T, was isolated from a patient with pulmonary metastases. The DNA GC content of the type strain is 67.2 mol%. The second strain, HKU78, was isolated from a patient with community acquired pneumonia. The DNA GC content of HKU78 is 67.1 mol%. The third strain, HKU79, was isolated from a patient with underlying Graves disease and paranoid schizophrenia. The DNA GC content of HKU79 is 67.2 mol%.
References
- Li ZJ, Zhang HY, Ren LL, Lu QB, Ren X, Zhang CH, et al.; Chinese Centers for Disease Control and Prevention (CDC) Etiology of Respiratory Infection Surveillance Study Team. Etiological and epidemiological features of acute respiratory infections in China. Nat Commun. 2021;12:5026. DOIPubMedGoogle Scholar
- Marusić A, Katalinić-Janković V, Popović-Grle S, Janković M, Mazuranić I, Puljić I, et al. Mycobacterium xenopi pulmonary disease - epidemiology and clinical features in non-immunocompromised patients. J Infect. 2009;58:108–12. DOIPubMedGoogle Scholar
- Munson E, Carella A, Carroll KC. Valid and accepted novel bacterial taxa derived from human clinical specimens and taxonomic revisions published in 2022. J Clin Microbiol. 2023;61:
e0083823 . DOIPubMedGoogle Scholar - Woo PC, Lau SK, Teng JL, Tse H, Yuen KY. Then and now: use of 16S rDNA gene sequencing for bacterial identification and discovery of novel bacteria in clinical microbiology laboratories. Clin Microbiol Infect. 2008;14:908–34. DOIPubMedGoogle Scholar
- Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing: thirty-fourth informational supplement (M100–ED34), Wayne (PA): The Institute; 2024.
- Hermankova K, Kourilova X, Pernicova I, Bezdicek M, Lengerova M, Obruca S, et al. Complete genome sequence of the type strain Tepidimonas taiwanensis LMG 22826T, a thermophilic alkaline protease and polyhydroxyalkanoate producer. Genome Biol Evol. 2021;13:evab280. DOIGoogle Scholar
- Albuquerque L, Castelhano N, Raposo P, Froufe HJC, Tiago I, Severino R, et al. Comparative genome sequence analysis of several species in the genus Tepidimonas and the description of a novel species Tepidimonas charontis sp. nov. Int J Syst Evol Microbiol. 2020;70:1596–604. DOIPubMedGoogle Scholar
- Woo PC, Leung KW, Tsoi HW, Wong SS, Teng JL, Yuen KY. Thermo-tolerant Campylobacter fetus bacteraemia identified by 16S ribosomal RNA gene sequencing: an emerging pathogen in immunocompromised patients. J Med Microbiol. 2002;51:740–6. DOIPubMedGoogle Scholar
- Chou YJ, Sheu SY, Sheu DS, Wang JT, Chen WM. Schlegelella aquatica sp. nov., a novel thermophilic bacterium isolated from a hot spring. Int J Syst Evol Microbiol. 2006;56:2793–7. DOIPubMedGoogle Scholar
- Wei DQ, Yu TT, Yao JC, Zhou EM, Song ZQ, Yin YR, et al. Lysobacter thermophilus sp. nov., isolated from a geothermal soil sample in Tengchong, south-west China. Antonie Van Leeuwenhoek. 2012;102:643–51. DOIPubMedGoogle Scholar
- Alves MP, Rainey FA, Nobre MF, da Costa MS. Thermomonas hydrothermalis sp. nov., a new slightly thermophilic gamma-proteobacterium isolated from a hot spring in central Portugal. Syst Appl Microbiol. 2003;26:70–5. DOIPubMedGoogle Scholar
- Chen TL, Chou YJ, Chen WM, Arun B, Young CC. Tepidimonas taiwanensis sp. nov., a novel alkaline-protease-producing bacterium isolated from a hot spring. Extremophiles. 2006;10:35–40. DOIPubMedGoogle Scholar
- Dhawan B, Sebastian S, Malhotra R, Kapil A, Gautam D. Prosthetic joint infection due to Lysobacter thermophilus diagnosed by 16S rRNA gene sequencing. Indian J Med Microbiol. 2016;34:100–2. DOIPubMedGoogle Scholar
- Ju JH, Kim JS, Lee DH, Jeon JH, Heo SY, Seo JW, et al. Thermomonas aquatica sp. nov., isolated from an industrial wastewater treatment plant. Int J Syst Evol Microbiol. 2019;69:3399–404. DOIPubMedGoogle Scholar
- Wu XT, He YQ, Li GX, Xiao H, Dai XR, Yang MR, et al. Genome sequence of sulfide-dependent denitrification bacterium Thermomonas sp. strain XSG, isolated from marine sediment. Microbiol Resour Announc. 2021;10:e00057–21. DOIPubMedGoogle Scholar
- Xu S, Chen J, Chen S, Lai Q, Liu Z, Xu Y. Thermomonas mangrovi sp. nov., isolated from soil of a mangrove nature reserve. Int J Syst Evol Microbiol. 2023;73:5. DOIPubMedGoogle Scholar
- Wang L, Zheng S, Wang D, Wang L, Wang G. Thermomonas carbonis sp. nov., isolated from the soil of a coal mine. Int J Syst Evol Microbiol. 2014;64:3631–5. DOIPubMedGoogle Scholar
- Kim MK, Im WT, In JG, Kim SH, Yang DC. Thermomonas koreensis sp. nov., a mesophilic bacterium isolated from a ginseng field. Int J Syst Evol Microbiol. 2006;56:1615–9. DOIPubMedGoogle Scholar
- Viana MC, Curty G, Furtado C, Singh B, Bendall ML, Viola JPB, et al. Naso-oropharyngeal microbiome from breast cancer patients diagnosed with COVID-19. Front Microbiol. 2023;13:
1074382 . DOIPubMedGoogle Scholar - Hemmi J, Makino S, Yokoo T, Kano H, Asami Y, Takeda K, et al. Consumption of yogurt fermented with Lactobacillus delbrueckii ssp. bulgaricus OLL1073R-1 augments serum antibody titers against seasonal influenza vaccine in healthy adults. Biosci Microbiota Food Health. 2023;42:73–80. DOIPubMedGoogle Scholar
- Neonakis IK, Skamagkas I, Stafylaki D, Maraki S. Lactobacillus delbrueckii urinary tract infection in a male patient: a case report. Germs. 2022;12:304–7. DOIPubMedGoogle Scholar
- Maillet F, Passeron A, Podglajen I, Ranque B, Pouchot J. Lactobacillus delbrueckii urinary tract infection in a male patient. Med Mal Infect. 2019;49:226–8. DOIPubMedGoogle Scholar
- Darbro BW, Petroelje BK, Doern GV. Lactobacillus delbrueckii as the cause of urinary tract infection. J Clin Microbiol. 2009;47:275–7. DOIPubMedGoogle Scholar
- Duprey KM, McCrea L, Rabinowitch BL, Azad KN. Pyelonephritis and bacteremia from Lactobacillus delbrueckii. Case Rep Infect Dis. 2012;2012:
745743 . DOIPubMedGoogle Scholar - Shimada T, Ishikawa K, Kawai F, Yoneoka D, Mori N. Risk factors associated with infection-related mortality of Bacillus cereus bacteremia in hematologic disorders. Int J Hematol. 2023;118:726–30. DOIPubMedGoogle Scholar
- Castedo E, Castro A, Martin P, Roda J, Montero CG. Bacillus cereus prosthetic valve endocarditis. Ann Throac Surg. 1999;68:2351–2. DOIGoogle Scholar
- Moreira C, Rainey FA, Nobre MF, da Silva MT, da Costa MS. Tepidimonas ignava gen. nov., sp. nov., a new chemolithoheterotrophic and slightly thermophilic member of the beta-Proteobacteria. Int J Syst Evol Microbiol. 2000;50:735–42. DOIPubMedGoogle Scholar
- Ko KS, Lee NY, Oh WS, Lee JH, Ki HK, Peck KR, et al. Tepidimonas arfidensis Sp. Nov., a Novel Gram-negative and thermophilic bacterium isolated from the bone marrow of a patient with leukemia in Korea. Microbiol Immunol. 2005;49:785–8. DOIPubMedGoogle Scholar
- Carnes MU, Siddiqui NY, Karstens L, Gantz MG, Dinwiddie DL, Sung VW, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network. Urinary microbiome community types associated with urinary incontinence severity in women. Am J Obstet Gynecol. 2024;230:344.e1–20. DOIPubMedGoogle Scholar
- Richter HE, Carnes MU, Komesu YM, Lukacz ES, Arya L, Bradley M, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Pelvic Floor Disorders Network. Association between the urogenital microbiome and surgical treatment response in women undergoing midurethral sling operation for mixed urinary incontinence. Am J Obstet Gynecol. 2022;226:93.e1–15. DOIPubMedGoogle Scholar
- Wessels JM, Domínguez MA, Leyland NA, Agarwal SK, Foster WG. Endometrial microbiota is more diverse in people with endometriosis than symptomatic controls. Sci Rep. 2021;11:18877. DOIPubMedGoogle Scholar
- Denoth L, Juillerat P, Kremer AE, Rogler G, Scharl M, Yilmaz B, et al.; On Behalf Of The Swiss Ibd Cohort Study. on behalf ff the Swiss Ibd Cohort Study. Modulation of the mucosa-associated microbiome linked to the PTPN2 risk gene in patients with primary sclerosing cholangitis and ulcerative colitis. Microorganisms. 2021;9:1752. DOIPubMedGoogle Scholar
- Kim JH, Kim SH, Lim JY, Kim D, Jeong IS, Lee DK, et al. Association between the sinus microbiota with eosinophilic inflammation and prognosis in chronic rhinosinusitis with nasal polyps. Exp Mol Med. 2020;52:978–87. DOIPubMedGoogle Scholar
- Freitas M, Rainey FA, Nobre MF, Silvestre AJ, da Costa MS. Tepidimonas aquatica sp. nov., a new slightly thermophilic beta-proteobacterium isolated from a hot water tank. Syst Appl Microbiol. 2003;26:376–81. DOIPubMedGoogle Scholar
- Gao R, Hu Y, Li Z, Sun J, Wang Q, Lin J, et al. Dissemination and mechanism for the MCR-1 colistin resistance. PLoS Pathog. 2016;12:
e1005957 . DOIPubMedGoogle Scholar - Sun J, Li XP, Fang LX, Sun RY, He YZ, Lin J, et al. Co-occurrence of mcr-1 in the chromosome and on an IncHI2 plasmid: persistence of colistin resistance in Escherichia coli. Int J Antimicrob Agents. 2018;51:842–7. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleOriginal Publication Date: January 23, 2026
Table of Contents – Volume 32, Number 1—January 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Kwok-Yung Yuen, Department of Microbiology, School of Clinical Medicine, Li Ka Shing Faculty of Medicine, University of Hong Kong, Daniel & Mayce Yu Administration Wing, 21 Sassoon Rd, Pokfulam, Hong Kong, China
Top