Volume 32, Number 2—February 2026
Dispatch
Temporal Clustering of Mycoplasma pneumoniae–Associated Encephalitis and Stroke, South Korea, 2024
Cite This Article
Citation for Media
Abstract
Seventeen pediatric encephalitis (n = 12) or stroke (n = 5) cases clustered temporally during the 2023–2024 Mycoplasma pneumoniae epidemic in South Korea; similar patterns had not been noted in previous seasons. Those findings might reflect postpandemic changes in clinical manifestation and underscore the need for neurologic surveillance during M. pneumoniae epidemics.
Mycoplasma pneumoniae is a major cause of community-acquired pneumonia in children and can also lead to extrapulmonary complications affecting multiple organ systems, including the central nervous system (CNS) (1,2). Neurologic complications, including encephalitis and stroke, are clinically consequential because of their severity and sequelae.
During the COVID-19 pandemic, nonpharmaceutical interventions markedly reduced the circulation of common respiratory pathogens, including M. pneumoniae (3). However, since 2023, a resurgence of M. pneumoniae has been reported worldwide (4). Amid this resurgence, we observed increased numbers of pediatric encephalitis and ischemic stroke cases associated with M. pneumoniae in South Korea during the 2023–2024 season (5). To better characterize that phenomenon, we analyzed the clinical features and outcomes of affected children and evaluated institutional and national surveillance data to place those findings in broader temporal and epidemiologic contexts.
We conducted a retrospective study of children hospitalized with encephalitis or ischemic stroke at 2 tertiary hospitals (center A, Seoul; center B, Seongnam) and 1 secondary care hospital (center C, Seoul) during the October 2023–December 2024 M. pneumoniae epidemic in South Korea, as defined by the Korea Disease Control and Prevention Agency surveillance program (Appendix Figure 1). M. pneumoniae infection was confirmed by using PCR of respiratory samples or by using serology (particle agglutination titer >1:160 or IgM index >1.4 by using enzyme-linked immunosorbent assay) (6). We defined encephalitis as an altered mental status lasting >24 hours with supportive tests and stroke as focal deficits with radiographic infarctions.
Figure 1

Figure 1. Monthly pediatric stroke and encephalitis cases (stacked bars) and Mycoplasma pneumoniaeinfections (green line) on the basis of aggregated data obtained from 3 hospitals in South Korea, October 2023–December...
We identified 17 cases of M. pneumoniae–associated encephalitis (n = 12) or ischemic stroke (n = 5). Of those cases, 13 occurred at center A, 4 at center B, and none at center C. Most cases were clustered during June–December 2024, which coincided with a marked increase in M. pneumoniae infections (Figure 1).
The median patient was 8.8 years of age; 52.9% of the patients were male and 47.1% female. Although 4 patients had no preceding respiratory symptoms, pneumonia was documented in 11 patients. The median interval from respiratory to neurologic symptom onset was 3 days (range 2–8 days). M. pneumoniae infection was confirmed in all 17 patients; 10 cases were confirmed by using both PCR (respiratory specimens) and serology, 6 cases by using serology, and 1 by using PCR (respiratory specimen). Cerebrospinal fluid PCR was performed on samples from 2 patients (1 positive case and 1 indeterminate case), and cerebrospinal fluid serology for M. pneumoniae was not performed. No other infectious or autoimmune etiologies were detected in the 17 patients. All 5 stroke patients had large-vessel infarctions in the middle cerebral artery or anterior cerebral artery territories; moreover, the clinical manifestations of 4 patients included multiterritorial involvement. Brain magnetic resonance imaging abnormalities (typically involving diffusion restriction or T2-weighted fluid-attenuated inversion recovery hyperintensities in the hippocampus, basal ganglia, or thalamus) were identified in 42% of the encephalitis patients.
Seven patients required intensive care unit admission. Twelve patients received intravenous antimicrobial drugs and 9 received corticosteroids; in addition, intravenous immunoglobulin was administered to 4 encephalitis patients. The outcomes were favorable; at the last follow-up, 83.3% of encephalitis and 60.0% of stroke patients demonstrated a modified Rankin scale score <2 (0–2 = no to mild disability), and no deaths were reported (Appendix Table 1).
During the same period (October 2023–December 2024), we identified 193 M. pneumoniae–associated hospitalizations without CNS involvement at the 3 hospitals for comparison. The median age and proportion of male patients were similar between the groups; however, the CNS complication group demonstrated substantially longer hospital stays (29 vs. 6 days; p<0.001) and a higher intensive care unit admission rate (41% vs. 3%; p<0.001) (Appendix Table 2).
Figure 2

Figure 2. Annual trends in pediatric Mycoplasma pneumoniae–associated admissions and central nervous system complications in South Korea. A) Data obtained from 3 hospitals during 2011–2024. Bars represent ischemic stroke and...
Figure 3
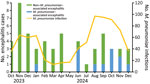
Figure 3. Monthly encephalitis cases by Mycoplasma pneumoniae association during the 2023–2024 epidemic, with concurrent M. pneumoniaeinfections (October 2023–December 2024). The bars show monthly encephalitis hospitalizations aggregated across...
We analyzed data from 2011–2024 to evaluate long-term trends in pediatric stroke, encephalitis, and M. pneumoniae–associated hospitalizations, which were identified by using administrative diagnostic codes from standardized clinical data warehouse records; in addition, we normalized annual case counts by total pediatric admissions for comparison. At the institutional level, the stroke and encephalitis rates did not consistently align with M. pneumoniae epidemic activity; however, both rates increased after 2020, possibly reflecting broader effects of the COVID-19 pandemic and its aftermath (Figure 2, panel A). In contrast, a distinct temporal overlap emerged in 2024; during June–December, M. pneumoniae infections accounted for 20%–100% of monthly encephalitis admissions across sites (Figure 3), suggesting a temporal association between M. pneumoniae circulation and neurologic complications during the epidemic.
We assessed nationwide trends in M. pneumoniae-associated admissions, encephalitis, and pediatric stroke from public datasets. We obtained M. pneumoniae–associated hospitalization data from the Korea Disease Control and Prevention Agency sentinel surveillance program (5), pediatric stroke data from the Korean Statistical Information Service (7), and nationwide encephalitis data from health insurance claims, excluding cases with confirmed pathogens (8). The incidence of encephalitis (all ages) remained stable from 2015–2019, with no apparent temporal association being detected with M. pneumoniae activity. In addition, the pediatric stroke data obtained from 2017–2021 did not demonstrate a temporal relationship with monthly M. pneumoniae activity (Figure 2, panel B).
The absence of temporal associations during previous epidemics contrasts with the clear increase in M. pneumoniae–associated CNS cases in 2024. That pattern might be partially explained by the immunity gap hypothesis (9), whereby prolonged suppression of respiratory pathogens during COVID-19 nonpharmaceutical interventions increased pediatric susceptibility, which is consistent with shifts in age distribution and disease severity reported in other studies (10,11). M. pneumoniae neurologic complications might result from direct CNS invasion, immune-mediated damage, and cerebrovascular occlusion (12). In this context, an increase in primary M. pneumoniae infections among seronegative children during 2023–2024 plausibly increased the risk for immune-mediated CNS complications; however, that relationship warrants further investigation. Moreover, strain features might contribute to increased severity; in 2023–2024, several studies reported P1 type 1 predominance and widespread A2063G macrolide resistance, accompanied by a high proportion of severe pulmonary manifestations (13,14). Strains exhibiting greater neurotropism might have been circulating during this period, although further validation is needed. Increased clinical awareness and the large scale of the epidemic might have increased the absolute number of rare complications.
The first limitation of this study is that the use of serologic testing to confirm M. pneumoniae infection reveals known constraints, including potential false positivity, delayed antibody responses, and interassay variability. Second, nationwide datasets lacked monthly resolution and pediatric detail and originated from different sources (the Korean Statistical Information Service and insurance claims data), limiting comparability. Finally, the absence of pathogen characterization precluded the evaluation of strain-specific factors potentially associated with neurologic complications.
Despite those limitations, our study provides clinical data highlighting increased pediatric CNS manifestations of M. pneumoniae infection observed during the 2023–2024 epidemic. In contrast to prior years, we observed a distinct temporal clustering of M. pneumoniae–associated CNS manifestations in South Korea in 2024. It is unclear whether the observed pattern reflects diagnostic capacity, heightened clinical vigilance, or a true shift in disease dynamics potentially driven by host, pathogen, or environmental factors. Further large-scale and longitudinal studies are warranted to determine whether this clustering represents an isolated event or signals an emerging trend in pediatric infectious diseases. Our findings underscore the importance of sustained epidemiologic surveillance and molecular characterization of circulating strains to better elucidate the mechanisms underlying extrapulmonary complications of M. pneumoniae infection.
Dr. Song is a clinical assistant professor in the Department of Pediatrics, Division of Infectious Diseases, SMG-SNU Boramae Medical Center, Seoul, South Korea. Her research interests include pediatric respiratory infections, including M. pneumoniae and respiratory syncytial virus.
References
- Waites KB, Xiao L, Liu Y, Balish MF, Atkinson TP. Mycoplasma pneumoniae from the respiratory tract and beyond. Clin Microbiol Rev. 2017;30:747–809. DOIPubMedGoogle Scholar
- Narita M. Pathogenesis of extrapulmonary manifestations of Mycoplasma pneumoniae infection with special reference to pneumonia. J Infect Chemother. 2010;16:162–9. DOIPubMedGoogle Scholar
- Chow EJ, Uyeki TM, Chu HY. The effects of the COVID-19 pandemic on community respiratory virus activity. Nat Rev Microbiol. 2023;21:195–210.PubMedGoogle Scholar
- Meyer Sauteur PM, Beeton ML, Pereyre S, Bébéar C, Gardette M, Hénin N, et al.; European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Mycoplasma and Chlamydia Infections (ESGMAC), and the ESGMAC Mycoplasma pneumoniae Surveillance (MAPS) study group. Mycoplasma pneumoniae: delayed re-emergence after COVID-19 pandemic restrictions. Lancet Microbe. 2024;5:e100–1. DOIPubMedGoogle Scholar
- Korea Disease Control and Prevention Agency. Acute respiratory infections surveillance system. 2025 [cited 2025 Aug 22]. https://dportal.kdca.go.kr/pot/is/st/ari.do
- Kim G, Yun KW, Kang D, Lee TJ, Eun BW, Lee H, et al. Diagnostic accuracy of serological tests for Mycoplasma pneumoniae infections in children with pneumonia, based on symptom onset. Ann Lab Med. 2025. DOIGoogle Scholar
- Korean Statistical Information Service. National stroke-related hospitalization statistics [cited 2025 Aug 22]. https://kosis.kr/index/index.do
- Kim SH, Baek JY, Han M, Lee M, Lim SM, Lee JY, et al. A decrease in the incidence of encephalitis in South Korea during the COVID-19 pandemic: A nationwide study between 2010 and 2021. J Med Virol. 2023;95:
e28490 . DOIPubMedGoogle Scholar - Cohen R, Ashman M, Taha M-K, Varon E, Angoulvant F, Levy C, et al. Pediatric Infectious Disease Group (GPIP) position paper on the immune debt of the COVID-19 pandemic in childhood, how can we fill the immunity gap? Infect Dis Now. 2021;51:418–23. DOIPubMedGoogle Scholar
- Dungu KHS, Holm M, Hartling U, Jensen LH, Nielsen AB, Schmidt LS, et al. Mycoplasma pneumoniae incidence, phenotype, and severity in children and adolescents in Denmark before, during, and after the COVID-19 pandemic: a nationwide multicentre population-based cohort study. Lancet Reg Health Eur. 2024;47:
101103 . DOIPubMedGoogle Scholar - You J, Zhang L, Chen W, Wu Q, Zhang D, Luo Z, et al. Epidemiological characteristics of mycoplasma pneumoniae in hospitalized children before, during, and after COVID-19 pandemic restrictions in Chongqing, China. Front Cell Infect Microbiol. 2024;14:
1424554 . DOIPubMedGoogle Scholar - Narita M. Pathogenesis of neurologic manifestations of Mycoplasma pneumoniae infection. Pediatr Neurol. 2009;41:159–66. DOIPubMedGoogle Scholar
- Chen Y, Li X, Fu Y, Yu Y, Zhou H. Whole-genome sequencing unveils the outbreak of Mycoplasma pneumoniae in mainland China. Lancet Microbe. 2024;5:
100870 . DOIPubMedGoogle Scholar - Xu L, Wang P, Wang Y, Liu B, Xu X, Yang Q, et al. Epidemiological, clinical, and genotypic characteristics of pediatric Mycoplasma pneumoniae infections: an 8-year survey in Suzhou, China in the pre- and post-COVID-19 eras. Front Microbiol. 2024;15:
1483152 . DOIPubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: February 15, 2026
Table of Contents – Volume 32, Number 2—February 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Ki Wook Yun, Department of Pediatrics, Seoul National University Children’s Hospital, 101, Daehak-ro Jongno-gu, 03080, South Korea
Top