Life-Threatening SARS-CoV-2–Associated Encephalopathy and Multiorgan Failure in Children, Asia and Oceania, 2022–2024
Mariko Kasai
1, Hiroshi Sakuma

, Motomasa Suzuki
1, Masahiro Nishiyama
1, Nanako Kawata
1, Jainn-Jim Lin
1, Kuang-Lin Lin, Velda Han, Shekeeb S. Mohammad, Russell C. Dale, Terrence Thomas, Kazuhiro Muramatsu, Osamu Mitani, Yoshiyuki Kobayashi, Kouhei Ishida, Yuichi Abe, Ichiro Kuki, and Jun-ichi Takanashi
Author affiliation: Tokyo Metropolitan Institute of Medical Science, Tokyo, Japan (M. Kasai, H. Sakuma); Aichi Children's Health and Medical Center, Aichi, Japan (M. Suzuki); Hyogo Prefectural Kobe Children’s Hospital, Kobe, Japan (M. Nishiyama); Tokyo Metropolitan Children’s Medical Center, Tokyo (N. Kawata); Chang Gung Children’s Hospital and Chang Gung Memorial Hospital, School of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan (J.-J. Lin, K.-L. Lin); Khoo Teck Puat-National University Children’s Medical Institute, Singapore (V. Han); Yong Loo Lin School of Medicine, National University of Singapore, Singapore (V. Han); Kids Neuroscience Centre, The Children’s Hospital at Westmead, Faculty of Medicine and Health, University of Sydney, Westmead, New South Wales, Australia (V. Han, S.S. Mohammad, R.C. Dale); KK Women’s and Children’s Hospital, Singapore (T. Thomas); Jichi Medical University, Tochigi, Japan (K. Muramatsu); Fukuyama City Hospital, Hiroshima, Japan (O. Mitani); Hiroshima University Hospital, Hiroshima (Y. Kobayashi); Sapporo Medical University School of Medicine, Sapporo, Japan (K. Ishida); National Center for Child Health and Development, Tokyo (Y. Abe); Osaka City General Hospital, Osaka, Japan (I. Kuki); Tokyo Women’s Medical University Yachiyo Medical Center, Chiba, Japan (J. Takanashi)
Main Article
Figure 2
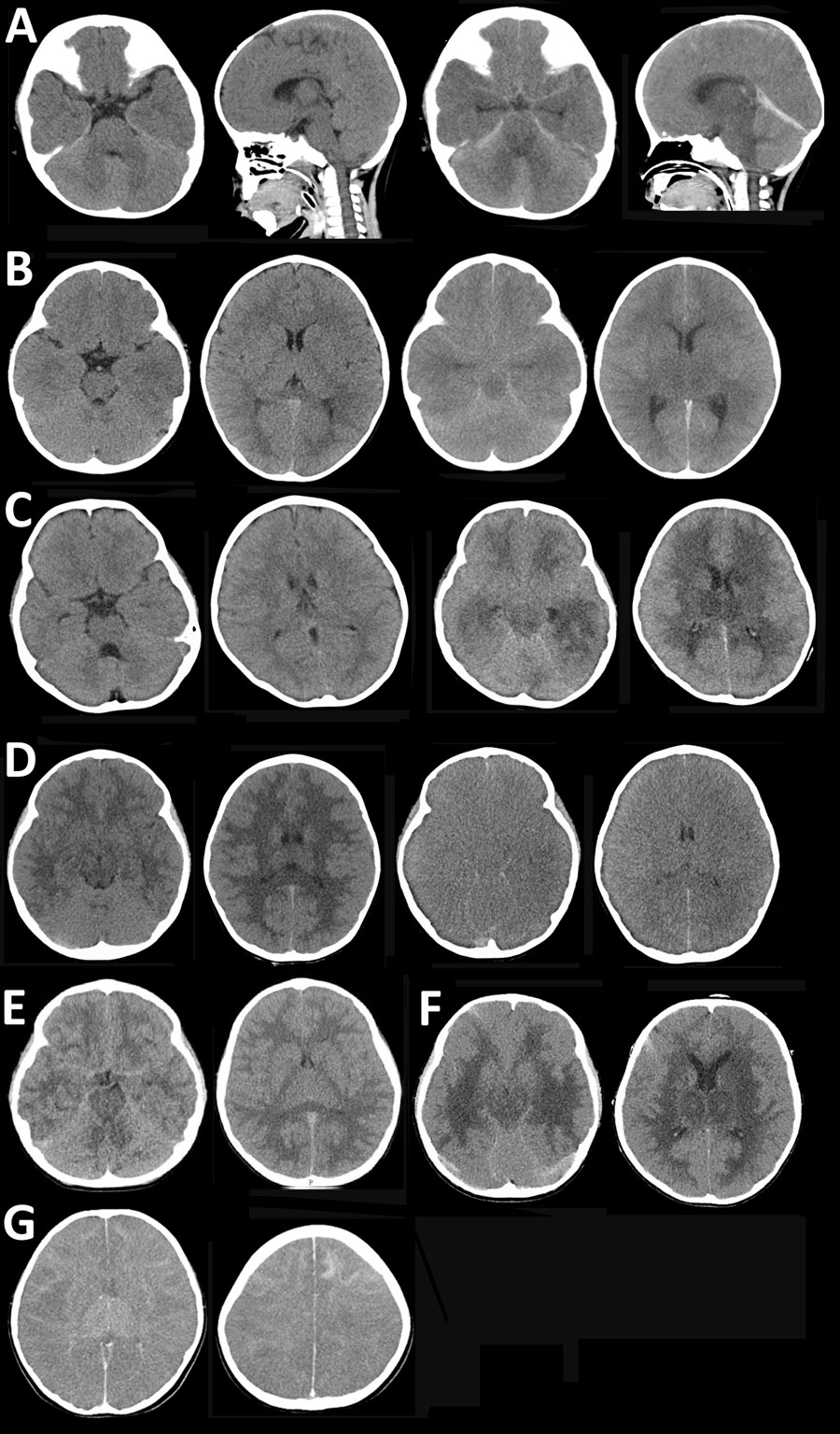
Figure 2. Brain computed tomography imaging for patients with SARS-CoV-2 acute shock with encephalopathy and multiorgan failure/acute fulminant cerebral edema (ASEM/AFCE) for study of life-threatening SARS-CoV-2–associated encephalopathy and multiorgan failure in children, Asia and Oceania, 2022–2024. A) Case-patient 1, showing diffuse cerebral edema (DCE) within 10 hours after onset of neurologic symptoms (left 2 images) and severe DCE and herniation at 18 hours after onset (right 2 images). B) Case-patient 6, showing mild cerebral edema within 4 hours after onset (left 2 images) and severe DCE at 23 hours after onset (right 2 images). C) Case-patient 15, showing DCE 3 hours after onset (left 2 images) and severe DCE with low-density involving the bilateral cerebral white matter and thalamus at 23 hours from the onset (right 2 images). D) Case-patient 19, showing DCE with low-density lesions in the bilateral cerebral white matter within 90 minutes after onset (left 2 images) and severe DCE at 10 hours after onset (right 2 images). E) Case-patient 18, showing mild cerebral edema on day 2 of illness; the patient had no further exacerbation of DCE. F) Case-patent 20, showing DCE with bilateral low-density lesions in the thalamus (left image) and periventricular cerebral white matter within 30 hours after onset (right image). G) Case-patient 23, showing DCE within 7 hours after onset (left image) and a high density of frontal subcortical white matter (right image).
Main Article
Page created: January 22, 2026
Page updated: February 19, 2026
Page reviewed: February 19, 2026
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.