Volume 32, Number 2—February 2026
Research
Predictors of Fatal Outcomes among Pediatric Patients Hospitalized for Rocky Mountain Spotted Fever, Sonora, Mexico, 2004–20241
Cite This Article
Citation for Media
Abstract
The tickborne disease Rocky Mountain spotted fever (RMSF) remains life-threatening among children in northern Mexico. We retrospectively investigated 500 pediatric RMSF patients hospitalized in Sonora during 2004–2024. We analyzed clinical, laboratory, and sociodemographic data to identify predictors of fatality by using descriptive statistics and multivariable logistic regression. We found that the overall case-fatality rate was 19.8%, decreasing over time from 31.4% (2004–2013) to 14.5% (2014–2024). Fatal outcomes were associated with delayed doxycycline treatment (>5 days after symptom onset), older age, Indigenous background, and abnormal laboratory markers. Among survivors, 16% had life-altering sequelae, including amputations and neurologic deficits. Cases occurred year-round, predominantly in urban settings. Timely doxycycline administration remains a critical factor in reducing mortality rates. Vulnerable populations, including persons living in poverty, children >10 years of age, and Indigenous communities, require targeted interventions. Strengthening early diagnosis and understanding mechanisms underlying severe disease and death could improve RMSF outcomes in endemic regions.
Rocky Mountain spotted fever (RMSF) is a severe, often fatal tickborne disease caused by Rickettsia rickettsii bacteria (1). Although multiple hard tick species carry R. rickettsii, the brown dog tick (Rhipicephalus sanguineus sensu lato) has emerged as the predominant vector in the southwestern United States and in Mexico (2,3). RMSF is associated with high case-fatality rates (CFRs), particularly in communities with lower socioeconomic status where close contact with tick-infested dogs is common (4).
RMSF is endemic in the Americas (1). During 2009–2023, Mexico reported 9,153 cases of spotted fever rickettsioses (SFR), including RMSF, nearly half of which occurred in US-bordering states. The state of Sonora had the highest CFR of the region; 37.9% of patients died from their infections (5), exceeding the 24% CFRs in the United States in the preantibiotic era (6), and far exceeding current US CFR estimates of 5%–10% (7). Of note, in Sonora, children accounted for more than half of confirmed RMSF cases and more than one quarter of deaths (5).
Without prompt doxycycline treatment, RMSF can rapidly progress to multiorgan failure and death; survivors can experience life-altering sequelae, including neurologic deficits or limb amputations (7,8). Treatment delays of >5 days from symptom onset triple the risk for death (8). Early symptoms, including fever, malaise, headache, and rash, are nonspecific and resemble other diseases like dengue and COVID-19 (9,10). Diagnostic limitations further complicate timely treatment: indirect immunofluorescent antibody (IFA) testing often requires send-out testing and confirmation of paired acute and convalescent samples (11), which typically takes days to weeks; PCR lacks sensitivity (12); and immunohistochemical (IHC) staining is not widely available and requires collection of tissue, often a punch biopsy of a rash lesion (13).
Previous studies identified clinical predictors of fatal outcomes in children, including septic shock, acute kidney injury, neurologic complications, hemorrhages, and hemophagocytic lymphohistiocytosis (8,14,15). Treatment-related factors, such as mechanical ventilation, inotropic support, intravenous fluid supplementation, and delayed doxycycline administration, also contribute to adverse outcomes (16). Although those aspects have been researched in Sonora (8,10,17), how clinical manifestations, treatment, and outcomes of hospitalized pediatric patients have evolved over the past 2 decades remain unclear. We examined trends in pediatric RMSF case-patients hospitalized at Sonora’s main public pediatric hospital during 2004–2024 to describe clinical characteristics and identify predictors of severe and fatal outcomes that can inform strategies to improve outcomes for children infected with RMSF.
Data Collection
We conducted a retrospective analysis of medical records from all children hospitalized with suspected SFR at the primary public pediatric referral center in the state of Sonora, Hospital Infantil del Estado de Sonora (HIES), during January 2, 2004–December 31, 2024. Case-patients included those who had RMSF or SFR diagnoses and an acute illness of <2 weeks’ duration that was characterized by fever, headache or irritability, and a rash that might involve the palms and soles. We assigned patients codes A77.0 (Spotted fever due to Rickettsia rickettsii) or A77.9 (Spotted fever, unspecified) from the International Classification of Diseases, 10th Revision (ICD-10) (18), on the basis of final classification. Laboratory confirmation was established either through a single blood sample testing positive for R. rickettsii or Rickettsia spp. by PCR or by positive IgG titer >1:64 using IFA. When laboratory confirmation was not possible, we used clinical and epidemiologic criteria to support the diagnosis. We identified a total of 558 case-patients and excluded 58 case-patients for whom we were unable to confirm clinical, laboratory, or discharge diagnoses, yielding a total of 500 case-patients for analysis. Original data collection was approved by the Research Ethics Committee (registration no. 2869) of HIES (registration no. 003/23, approved June 20, 2023), and secondary analysis of de-identified data was determined to be nonhuman subjects research by the institutional review board of Emory University (Atlanta, GA, USA) on April 1, 2025.
HIES investigators trained in standardized chart review procedures and blinded to the study objectives extracted data from medical records. Extracted variables included clinical signs and symptoms, laboratory data at admission, sociodemographic variables, method of diagnostic confirmation, and factors related to medical care (e.g., day of symptom onset, day of doxycycline initiation), as well as discharge outcomes. The socioeconomic status (SES) variable represents an internal categorization by HIES, which primarily serves patients without any formal health insurance system affiliation, generally representing middle- and low-income populations. HIES classifies patients into 8 socioeconomic categories, which we dichotomized as having either sufficient or insufficient economic resources.
When available, we categorized patient weights and heights as moderately underweight if the weight-for-age was <2 SD below the median for sex and malnourished if body mass index (BMI) was <2 below SD the median for children >24 months of age or if weight-for-length was below the second percentile for children <24 months of age. We made those categorizations on the basis of World Health Organization International Growth Charts for children <24 months (19) and the US Centers for Disease Control and Prevention (CDC) Growth Charts for persons >24 months of age (20), as recommended by CDC (21). Because CDC charts report percentiles, we calculated the 2 SD threshold of weight by using the formula documented (22).
Data Analysis
We estimated annual cumulative incidence and mortality rates per million pediatric population from 2004–2024. The denominator for those calculations was the pediatric population (children 0–18 years of age) covered by the Ministry of Health, representing ≈32% of the total population. We calculated CFRs by using the number of deaths as the numerator and the number of confirmed case-patients at HIES as the denominator. We plotted polynomial-smoothed temporal trends for those epidemiologic indicators and assessed statistical significance by using the coefficient of determination (R2) and 95% CIs.
For statistical analysis, we primarily stratified study participants by case outcome (i.e., fatal or nonfatal) and period of occurrence (2004–2013 vs. 2014–2024). We additionally performed subanalyses, assessing disease severity by stratifying case-patients with long-term sequelae or death versus those whose disease resolved without sequelae, and among survivors, comparing those with long-term sequelae versus those without.
We used R version 4.5.0 (The R Project for Statistical Computing, https://www.r-project.org) to perform descriptive statistical analysis to evaluate the clinical characteristics of the study population. We assessed laboratory values both as continuous and categorical variables, classified as normal or abnormal on the basis of age-specific reference ranges (23). We used Kruskal-Wallis analysis of variance, Fisher exact test, and Pearson χ2 test to compare differences between groups. We considered p<0.05 statistically significant for all predictors except clinical symptoms and laboratory values, for which we considered p<0.001 significant, applying a Bonferroni correction for multiple comparisons (24).
We conducted bivariable and multivariable logistic regression analyses to assess associations between predictors and fatality and developed a multivariable model to evaluate sociodemographic and treatment-associated factors. To decrease collinearity, we selected predictors by choosing 1 representative variable per concept by lowest p value in bivariable analysis or, if all nonsignificant, least manipulated (e.g., continuous instead of categorical age) and excluded variables with >10 missing values. We entered all candidate variables into the model and assessed collinearity by using car package version 3.1-3 (all variance inflation factor <5; https://CRAN.R-project.org/package=car), followed by backward selection using the stepAIC function from MASS package version 7.3-65 (https://CRAN.R-project.org/package=MASS) to obtain the final model with the lowest Akaike information criteria (AIC). We also calculated adjusted odds ratios (aORs) and 95% CIs.
Figure 1

Figure 1. Incidence of cases and deaths per 1 million children and case-fatality rates over time in study of predictors of fatal outcomes among pediatric patients hospitalized for Rocky Mountain spotted fever,...
RMSF incidence at HIES rose steadily during 2004–2015, then fluctuated, with subsequent peaks in 2018 and 2022 (Figure 1, panel A). During the study period, 500 children were hospitalized with RMSF, and 372 (74.4%) had laboratory-confirmed RMSF. The overall CFR was 19.8% (99/500), decreasing from 31.4% (49/156) in 2004–2013 to 14.5% (50/344) in 2014–2024 (odds ratio [OR] 0.37 [95% CI 0.24–0.58]; p<0.001). CFR rose until the early 2010s, then declined modestly (R2 = 0.3326), with a relative increase after 2020. Mortality rates began to decline around 2013 and then stabilized at ≈20 deaths/1 million children served by the Ministry of Health annually (Figure 1, panel B).
In addition to the high mortality rates, 16% (n = 64) of survivors experienced severe, permanent sequelae, including amputations and neurologic impairment. Those outcomes declined from 25.3% (25/99) during 2004–2013 to 13% (39/301) during 2014–2024 (OR 0.50 [95% CI 0.29–0.89]; p = 0.016). Overall, 32.7% (163/499) of case-patients experienced either death or life-altering sequelae, a rate that nearly halved from 47.4% (74/156) during 2004–2013 to 25.9% (89/343) during 2014–2024.
Figure 2

Figure 2. Attack rates by municipality of residence in study of predictors of fatal outcomes among pediatric patients hospitalized for Rocky Mountain spotted fever, Sonora, Mexico, 2004–2024. Map created by Esri ArcGIS...
Case-patients were concentrated in central and southern Sonora, particularly in Hermosillo, the state capital and most populous city (Figure 2). We noted an urban predominance; 420 case-patients were from urban areas versus 80 from rural regions; however, fatality rates did not differ significantly by setting (p = 0.36) (Table 1). RMSF cases occurred year-round, and we did not note any seasonal or monthly patterns (Appendix Figure). In addition, most (93.5%) children had a documented history of tick exposure before hospitalization.
Sociodemographic Features
Slightly more case-patients were male (54%) than female (46%); we found no significant association between sex and fatality (p = 0.50) (Table 1). Most (87%) children were classified as having insufficient SES; ≈10% were of Indigenous origin, representing 10 ethnic groups, and most resided in impoverished suburban or rural communities. During 2014–2024, older age was significantly associated with higher CFR, and the median age among fatal cases was 10.3 (interquartile range [IQR] 6.9–14.2) years versus 8.5 (IQR 5.5–12.2) years in nonfatal cases (p = 0.048); that association was not observed across the full study period.
Clinical and Laboratory Features
Figure 3

Figure 3. Clinical progress of children in in study of predictors of fatal outcomes among pediatric patients hospitalized for Rocky Mountain spotted fever, Sonora, Mexico, 2004–2024. A) Maculopapular rash on the palm...
The most common clinical features at hospital admission were fever (100%); exanthema (95%) (Figure 3, panels A, B), notably on palms (81%) or soles (77%); and headache (88%) (Appendix Table 1). Features significantly (p<0.001 for all) associated with fatal outcomes were vomiting, petechial rash, hemorrhage, ecchymosis and necrosis (Figure 3, panels C, D), respiratory distress, pulmonary and peripheral edema, hepatomegaly, neurologic alterations (e.g., altered mental status, confusion, seizures, encephalitis, coma), hypovolemia, and shock (Appendix Table 1).
The most frequent abnormal laboratory findings, defined as values outside age-specific reference ranges (23), were procalcitonin (98%), aspartate aminotransferase (AST) (92%), lactate dehydrogenase (LDH) (91%), platelet count (85%), prothrombin time (PT) (85%), alanine aminotransferase (ALT) (81%), and serum sodium (81%) (Appendix Table 2). Nearly all laboratory parameters we assessed were significantly associated with fatality (p<0.001), including leukocytosis, neutrophilia, elevated neutrophil-to-lymphocyte ratio (NLR), thrombocytopenia, elevated procalcitonin, prolonged prothrombin time (PT) and partial thromboplastin time (PTT), elevated liver enzymes (AST, ALT, LDH), elevated creatinine, low albumin, and low total protein (Table 2). Although both fatal and nonfatal cases had many abnormal values, those values were markedly more severe in the fatal group; for example, the median platelet count was 17,000/µL in fatal cases versus 60,000/µL in nonfatal cases (reference range 150,000–450,000/µL) (Table 2).
Clinical Course and Outcomes
Figure 4
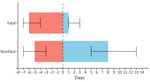
Figure 4. Analysis of days from symptom onset to hospitalization and length of hospital stay as predictors of fatal outcomes among pediatric patients hospitalized for Rocky Mountain spotted fever, Sonora, Mexico, 2004–2024....
Children with fatal outcomes were hospitalized later, at a median of 6 (IQR 4–7) days after symptom onset, compared with 5 (IQR 3–7) days in nonfatal cases (p<0.001) (Figure 4; Appendix Table 1). Children with later hospitalization times were also significantly more likely to develop complications during hospitalization, including vascular instability, secondary bacterial infections, neurologic disturbances, respiratory distress, acute renal failure, and shock (all p<0.001) (Table 3).
Doxycycline was administered at a median of 6 (IQR 5–7) days of illness in fatal cases versus 5 (IQR 3–7) days in nonfatal cases. Delayed treatment (>5 days) was significantly associated with death (p = 0.01) (Table 3). During 2014–2024, physicians more frequently initiated doxycycline within 5 days of symptom onset than during 2004–2013 (59% vs. 50%). Overall, 98% (490/500) of children received doxycycline during hospitalization, and 55% (276/500) received it within 5 days of symptom onset. Of the 10 children who did not receive doxycycline, 9 died and 1 survived; 2 of those children (both with fatal outcomes) were from Indigenous backgrounds, and the other 8 children (7 fatal with outcomes) were non-Indigenous. Of note, 40 children died despite receiving timely treatment, representing 40% of recorded deaths.
Multivariable Model
For the multivariable model, we assessed the following variables as potential predictors for death: sex, age, urbanicity, region, exposure to ticks, SES, Indigenous background, season (fall/winter/summer/spring), days of in-hospital treatment with doxycycline, time to doxycycline treatment, number of symptomatic days before hospital arrival, treatment with doxycycline monotherapy, and multidrug therapy. The best-fit model included ethnicity, days of in-hospital doxycycline treatment, time to doxycycline treatment, and doxycycline monotherapy (Table 4). After adjusting for other predictors, both a higher number of days from symptom onset to doxycycline treatment (aOR 1.19 [95% CI 1.08–1.31]) and Indigenous background (aOR 2.84 [95% CI 1.15–6.90]) were associated with higher odds of death. In contrast, doxycycline monotherapy (intravenous or oral) was protective (aOR 0.18 [95% CI 0.08–0.38]), as was more days of in-hospital doxycycline (aOR 0.63 [95% CI 0.57–0.69]) (Table 4).
Morbidity Subanalysis
Among hospitalized RMSF survivors, 64 (16%) were discharged with long-term sequelae, including neurologic impairments, amputations, and cardiac or respiratory complications. Children with long-term sequalae were more likely to be Indigenous (p = 0.006) and have delayed doxycycline treatment (p = 0.04) than children discharged without sequelae. Children with long-term sequalae also more frequently had rash on the palms or soles, petechiae, and signs of disease progression (e.g., hepatomegaly, neurologic signs, edema, and shock) (Appendix Table 3). Laboratory abnormalities were also more common in that group, and we noted statistically significant differences in platelet count, AST, LDH, serum albumin, and total protein levels (all p<0.001) (Appendix Table 4). As in fatal cases, children who survived with sequelae had a median time to doxycycline treatment of 6 days, but children without sequalae were treated at a median of 5 days (Appendix Table 3). Analyses combining sequelae and death as adverse outcomes yielded results similar to those observed when comparing fatal to nonfatal cases.
Our findings indicate that RMSF remains a major pediatric health concern among the population in Sonora, Mexico. Although the CFR declined to 14.5% during 2014–2024, it remains twice as high as that of neighboring Arizona, USA (7%), during 2008–2017 (25). However, CFR was lower than the 24.1% observed in Brazil (2007–2015) (26) and CFRs from other areas of Mexico, ranging from 20.2% (8) to 58.8% (27). In those regions, fatal outcomes are closely linked to a complex interplay of social and ecologic determinants, including limited access to healthcare (28) and high exposure to R. sanguineus–infected ticks, particularly among children living near large populations of free-roaming or stray dogs (29).
We found that one third of children in this study died or experienced long-term disability because of RMSF. That finding highlights the need to systematically incorporate severe sequelae into clinical assessments to more accurately estimate the true burden of RMSF in pediatric populations and to avoid underestimation when only considering in-hospital deaths (30). Our analysis also revealed a shift in the age-related risk for death and that children >10 years of age had increased fatality rates during the last decade of the study period. Historically, children <10 years of age were considered the most vulnerable to severe RMSF outcomes (31). Although the reasons for the shift remain unclear, increased awareness and clinician training, particularly regarding doxycycline safety in young children, might partially explain the trend. Further research is needed to explore specific vulnerabilities to RMSF among adolescents.
We also found significant associations between Indigenous background and negative outcomes, including both death and long-term sequelae. That finding could partially be related to lack of doxycycline administration among the population because a greater percentage of Indigenous versus non-Indigenous children (3.9% vs. 1.8%) received no doxycycline treatment. That disparity also could reflect a range of factors not fully captured in our dataset. Although Indigenous populations in Mexico have historically faced systemic inequities in health access and social services (32), further research should explore additional contributors to poor outcomes in that population, such as the regional presence of highly virulent R. rickettsii genetic clades (e.g., Taiaçu and Sheila Smith) (33), glucose-6-phosphate dehydrogenase deficiency (34), barriers within primary or nonreferral healthcare systems, and social determinants related to language, beliefs, and cultural practices (3,28,35). Those factors are particularly relevant given the annual migration of ≈160,000 agricultural workers, many from diverse Indigenous communities, from southern to northwest Mexico (36), including RMSF-endemic areas of Sonora.
Although 53% of RMSF cases occurred during July–October, Sonora’s warmest months, we observed no clear seasonal pattern in incidence or mortality rates, consistent with previous reports (37,38). Therefore, clinicians should maintain a high index of suspicion for RMSF year-round to ensure timely diagnosis and treatment (39). Furthermore, our findings indicate that RMSF in this pediatric population primarily occurs in urban foci, contrasting with the historically rural and suburban distribution of the disease (40,41). In both the southwestern United States and in Mexico, RMSF is strongly associated with large populations of tick-infested stray and domestic dogs, often concentrated in densely populated, low-income areas, thereby enabling exposure and transmission (29,42).
The most frequently observed clinical symptoms (fever, rash, and headache) were highly nonspecific, underscoring challenges clinicians face in establishing timely diagnosis and treatment. That finding highlights the urgent need for rapid and reliable diagnostic tools to support early clinical decision-making and prevent disease progression. Currently available methods for confirming RMSF, such as IFA, PCR, and IHC, are valuable for epidemiologic purposes but have limited clinical efficacy because of methodologic constraints and the need for specialized personnel and infrastructure (43,44). Therefore, strengthening laboratory capacity and developing new rapid diagnostics are essential not only for enhancing RMSF surveillance but also to guide clinical decision-making and improve outcomes in resource-limited settings (5,7,28).
We found that symptoms associated with fatal RMSF outcomes were predominantly related to disruptions in coagulation, vascular permeability, and neurologic function. Those clinical manifestations were supported by abnormal laboratory findings, such as thrombocytopenia, hyponatremia, and elevated liver enzymes and creatinine, consistent with previous studies (8,16,27,45). Although many laboratory abnormalities were noted in all case-patients, elevated neutrophil counts, increased NLR (46), prolonged PTT, elevated creatinine, hypoalbuminemia, and low total protein were significantly more frequent and severe in fatal cases (p<0.001) (Table 2; Appendix Table 2). Although recognized in other disease contexts (47), some of those biomarkers have not been consistently emphasized in the RMSF literature, suggesting their potential as underrecognized indicators of severe and fatal outcomes.
Comparing the clinical manifestations of fatal versus nonfatal cases and survivors with sequalae versus those who fully recovered, several notable trends emerged. As expected, laboratory abnormalities increased with disease severity. Platelet counts were markedly lower in fatal cases (median 17,000/µL) and in survivors with sequelae (median 22,000/µL) compared with fully recovered survivors (median 72,000/µL) (reference range 150,000–450,000/µL), suggesting platelet count could serve as a key marker of RMSF severity. Children discharged with sequelae and those who died also experienced significantly more severe symptoms and complications (e.g., edema, hemorrhage, shock) during hospitalization (p<0.001). Of note, case-patients who died more often experienced vomiting and showed substantial differences in PT, PTT, and NLR than those who survived, patterns not observed when comparing surviving case-patients with and without sequalae. Those findings could aid in clinical stratification of disease severity and identifying predictors of fatal outcomes.
Most of the statistically significant clinical signs we identified reflect the severity and rapid progression of RMSF, typically emerging after the fifth day of illness. That delayed clinical manifestation hindered timely intervention and increased the risk for fatal outcomes (48), underscoring the need for predictive tools to identify high-risk patients earlier. We propose developing a composite clinical severity score or a machine learning–based algorithm integrating early clinical indicators (e.g., vital signs, basic laboratory parameters, epidemiologic risk factors) to stratify patients at initial examination. Those tools should be built using retrospective clinical data and prospectively validated to ensure rigor and ethical application. Their implementation in endemic areas could substantially improve early diagnosis, guide timely treatment, and reduce RMSF-related fatality.
Our findings reinforce that early doxycycline initiation is critical for avoiding severe outcomes; we found administration beyond 5 days after symptom onset was a strong predictor of death, consistent with previous reports (3,8). That finding is particularly concerning because during the first decade of our study, half of case-patients received doxycycline after the 5-day threshold. Although the percentage receiving doxycycline >5 days after symptom onset declined to 41% during 2014–2024, delays remained common. Educational efforts targeting healthcare providers and community members appear to have improved timely doxycycline administration, especially in younger children (39); nevertheless, further action is needed to improve early recognition and treatment across all ages. Timeliness was also limited by delayed hospital arrival; median time from symptom onset to hospital arrival was 5 days, leaving a narrow window for intervention. Although whether case-patients sought care or received treatment before HIES admission is unclear, the need for 2 key strategies is evident: increasing awareness among primary care providers to initiate doxycycline earlier or refer patients to hospital care without delay, and implementing community-based programs encouraging caregivers to seek immediate care for children with suspected RMSF (5,28).
The first limitation of this retrospective study is the possibility for selection bias because the cohort included only patients treated at HIES, which primarily treats uninsured and severely ill patients, potentially limiting generalizability to the broader pediatric population affected by RMSF in Sonora. Second, information bias is also a concern because of variability in medical record quality and absence of prehospital care data, and because 25.5% (128/500) of case-patients were clinically diagnosed without laboratory confirmation. As described previously, laboratory confirmation is a pervasive problem for SFR globally, especially in resource-limited settings. Although laboratory confirmation is preferred to validate SFR cases (49), clinical manifestations of our identified case-patients aligned with studies published by CDC (2,7), supporting our conclusions of SFR diagnosis. Those limitations preclude causal inference; rather, our aim was to identify major predictors of fatal outcomes in pediatric RMSF and improve our understanding of its clinical and epidemiologic profile.
In summary, RMSF remains a major cause of severe pediatric illness and death in Sonora. Further research is needed to elucidate host, pathogen, and environmental determinants of RMSF-related mortality and long-term sequelae, especially among low-income communities, children >10 years, and Indigenous populations. Continued investment in diagnostic testing, education, and prevention is essential for reducing the burden of this treatable disease.
Dr. Bellman is a physician-scientist in training and postdoctoral researcher at Emory University and Children’s Healthcare of Atlanta. Her main interests include understanding the ecology and epidemiology of emerging infectious diseases and vectorborne diseases, and improving diagnostics for neglected tropical diseases.
Acknowledgment
We thank Christopher Paddock for his helpful expertise on RMSF and Grace Gombolay for her feedback on the clinical interpretation of results.
References
- Demma LJ, Traeger MS, Nicholson WL, Paddock CD, Blau DM, Eremeeva ME, et al. Rocky Mountain spotted fever from an unexpected tick vector in Arizona. N Engl J Med. 2005;353:587–94. DOIGoogle Scholar
- Álvarez-Hernández G, Roldán JFG, Milan NSH, Lash RR, Behravesh CB, Paddock CD. Rocky Mountain spotted fever in Mexico: past, present, and future. Lancet Infect Dis. 2017;17:e189–96. DOIGoogle Scholar
- Foley J, Tinoco-Gracia L, Rodriguez-Lomelí M, Estrada-Guzmán J, Fierro M, Mattar-Lopez E, et al. Unbiased assessment of abundance of Rhipicephalus sanguineus sensu lato ticks, canine exposure to spotted fever group Rickettsia, and risk factors in Mexicali, México. Am J Trop Med Hyg. 2019;101:22–32. DOIGoogle Scholar
- Álvarez-Hernández G, López-Ridaura R, Cortés-Alcalá R, García Rodríguez G, Calleja-López JRT, Rivera-Rosas CN, et al. Rocky Mountain spotted fever in Mexico: a call to action. Am J Trop Med Hyg. 2024;111:1070–7. DOIGoogle Scholar
- Dahlgren FS, Holman RC, Paddock CD, Callinan LS, McQuiston JH. Fatal Rocky Mountain spotted fever in the United States, 1999–2007. Am J Trop Med Hyg. 2012;86:713–9. DOIGoogle Scholar
- Biggs HM, Behravesh CB, Bradley KK, Dahlgren FS, Drexler NA, Dumler JS, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis—United States. MMWR Recomm Rep. 2016;65:1–44. DOIGoogle Scholar
- Alvarez-Hernandez G, Murillo-Benitez C, Candia-Plata Mdel C, Moro M. Clinical profile and predictors of fatal Rocky Mountain spotted fever in children from Sonora, Mexico. Pediatr Infect Dis J. 2015;34:125–30. DOIGoogle Scholar
- Mora JD, Licona-Enríquez JD, Álvarez-López DI, Aguilar-León DE, Álvarez-Hernández G. Clinical features of patients with Rocky Mountain spotted fever, dengue and chikungunya infection [in Spanish]. Gac Med Mex. 2021;157:58–63. DOIGoogle Scholar
- Álvarez-Hernández G, Rivera-Rosas CN, Calleja-López JRT, Álvarez-Meza JB, Candia-Plata MDC, Cruz-Loustaunau D, et al. A comparison of the clinical and epidemiological profile of Rocky Mountain spotted fever with dengue and COVID-19 in hospitalized children, Sonora, México, 2015–2022. Trop Med Infect Dis. 2025;10:20. DOIGoogle Scholar
- McQuiston JH, Wiedeman C, Singleton J, Carpenter LR, McElroy K, Mosites E, et al. Inadequacy of IgM antibody tests for diagnosis of Rocky Mountain spotted fever. Am J Trop Med Hyg. 2014;91:767–70. DOIGoogle Scholar
- Chung IH, Robinson LK, Stewart-Juba JJ, Dasch GA, Kato CY. Analytically sensitive Rickettsia species detection for laboratory diagnosis. Am J Trop Med Hyg. 2022;106:1352–7. DOIGoogle Scholar
- Paddock CD, Greer PW, Ferebee TL, Singleton J Jr, McKechnie DB, Treadwell TA, et al. Hidden mortality attributable to Rocky Mountain spotted fever: immunohistochemical detection of fatal, serologically unconfirmed disease. J Infect Dis. 1999;179:1469–76. DOIGoogle Scholar
- Nogueira Angerami R, Oliveira Morais E, Katz G, Jacintho da Silva L. Brazilian spotted fever in the paediatric age-segment in the state of São Paulo, southeastern Brazil, 2003–2006. Clin Microbiol Infect. 2009;15(Suppl 2):205–6. DOIGoogle Scholar
- Hosahalli Vasanna S, Lim PPC, Khan TS, Dalal J. Secondary hemophagocytic lymphohistiocytosis associated with Rocky Mountain spotted fever in a toddler: a case report. eJHaem. 2022;3:463–6. DOIGoogle Scholar
- Buckingham SC, Marshall GS, Schutze GE, Woods CR, Jackson MA, Patterson LE, et al.; Tick-borne Infections in Children Study Group. Clinical and laboratory features, hospital course, and outcome of Rocky Mountain spotted fever in children. J Pediatr. 2007;150:180-4–184.e1. DOIGoogle Scholar
- Álvarez-Hernández G, Candia-Plata MC, Delgado-de la Mora J, Acuña-Meléndrez NH, Vargas-Ortega AP, Licona-Enríquez JD. Rocky Mountain spotted fever in Mexican children: clinical and mortality factors [in Spanish]. Salud Publica Mex. 2016;58:385–92.
- World Health Organization. The ICD-10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva: The Organization; 1993.
- World Health Organization. Nutrition and Food Safety (NFS). WHO child growth standards: growth velocity based on weight, length and head circumference: methods and development, 1st ed. Geneva: The Organization; 2009.
- Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2002;246:1–190.
- Grummer-Strawn LM, Reinold C, Krebs NF; Centers for Disease Control and Prevention. Use of World Health Organization and CDC growth charts for children aged 0–59 months in the United States. MMWR Recomm Rep. 2010;59:1–15.
- Flegal KM, Cole TJ. Construction of LMS parameters for the Centers for Disease Control and Prevention 2000 growth charts. Natl Health Stat Rep. 2013;63:1–3.
- Children’s Hospital of Philadelphia Pathology & Laboratory Medicine. Laboratory reference ranges [cited 2025 Aug 5]. https://www.chop.edu/sites/default/files/2024-06/chop-labs-reference-ranges.pdf
- Armstrong RA. When to use the Bonferroni correction. Ophthalmic Physiol Opt. 2014;34:502–8. DOIGoogle Scholar
- Centers for Disease Control and Prevention. Data and statistics on spotted fever rickettsiosis [cited 2025 Aug 5]. https://www.cdc.gov/rocky-mountain-spotted-fever/data-research/facts-stats/index.html
- de Oliveira SV, Guimarães JN, Reckziegel GC, Neves BM, Araújo-Vilges KM, Fonseca LX, et al. An update on the epidemiological situation of spotted fever in Brazil. J Venom Anim Toxins Incl Trop Dis. 2016;22:22. DOIGoogle Scholar
- Estrada-Mendizabal RJ, Tamez-Rivera O, Vela EH, Blanco-Murillo P, Alanis-Garza C, Flores-Gouyonnet J, et al. Rickettsial disease outbreak, Mexico, 2022. Emerg Infect Dis. 2023;29:1944–7. DOIGoogle Scholar
- Álvarez-Hernández G, Paddock CD, Walker DH, Valenzuela JG, Calleja-López JRT, Rivera-Rosas CN, et al. Rocky Mountain spotted fever is a neglected tropical disease in Latin America. PLoS Negl Trop Dis. 2024;18:
e0012276 . DOIGoogle Scholar - Foley J, López-Pérez AM, Álvarez-Hernández G, Labruna MB, Angerami RN, Zazueta OE, et al. A wolf at the door: the ecology, epidemiology, and emergence of community- and urban-level Rocky Mountain spotted fever in the Americas. Am J Vet Res. 2025;86:12. DOIGoogle Scholar
- Laupland KB, Pasquill K, Parfitt EC, Dagasso G, Gupta K, Steele L. Inhospital death is a biased measure of fatal outcome from bloodstream infection. Clin Epidemiol. 2019;11:47–52. DOIGoogle Scholar
- Openshaw JJ, Swerdlow DL, Krebs JW, Holman RC, Mandel E, Harvey A, et al. Rocky Mountain spotted fever in the United States, 2000–2007: interpreting contemporary increases in incidence. Am J Trop Med Hyg. 2010;83:174–82. DOIGoogle Scholar
- Pelcastre-Villafuerte BE, Meneses-Navarro S, Sánchez-Domínguez M, Meléndez-Navarro D, Freyermuth-Encis G. Health conditions and use of services among indigenous peoples of Mexico [in Spanish]. Salud Publica Mex. 2020;62:810–9. DOIGoogle Scholar
- Brito-Lorán CB, Araiza-Rodríguez A, Garcés-Ayala F, Contreras-Pérez CU, Montes-Colima NA, López-Martínez I, et al. Analysis of Rocky Mountain spotted fever cases in northern Mexico reveals genetic variability of Rickettsia rickettsii and the different distribution of genotypes. Int Microbiol. 2023;27:689–95. DOIGoogle Scholar
- Walker DH, Kirkman HN. Rocky Mountain spotted fever and deficiency in glucose-6-phosphate dehydrogenase. J Infect Dis. 1980;142:771. DOIGoogle Scholar
- Alvarez-Hernandez G, Drexler N, Paddock CD, Licona-Enriquez JD, la Mora JD, Straily A, et al. Community-based prevention of epidemic Rocky Mountain spotted fever among minority populations in Sonora, Mexico, using a One Health approach. Trans R Soc Trop Med Hyg. 2020;114:293–300. DOIGoogle Scholar
- Velasco L, Coubes ML, Contreras OF. The vulnerability of migrant farmworkers and COVID-19 [in Spanish] [cited 2025 Aug 5]. https://www.colef.mx/noticia/la-vulnerabilidad-de-los-jornaleros-agricolas-migrantes-y-el-covid-19
- Zazueta OE, Armstrong PA, Márquez-Elguea A, Hernández Milán NS, Peterson AE, Ovalle-Marroquín DF, et al. Rocky Mountain spotted fever in a large metropolitan venter, Mexico–United States border, 2009–2019. Emerg Infect Dis. 2021;27:1567–76. DOIGoogle Scholar
- Álvarez-López DI, Ochoa-Mora E, Nichols Heitman K, Binder AM, Álvarez-Hernández G, Armstrong PA. Epidemiology and clinical features of Rocky Mountain spotted fever from enhanced surveillance, Sonora, Mexico: 2015–2018. Am J Trop Med Hyg. 2021;104:190–7. DOIGoogle Scholar
- Alvarez-Hernandez G, Ernst K, Acuña-Melendrez NH, Vargas-Ortega AP, Candia-Plata MDC. Medical knowledge related to Rocky Mountain spotted fever in Sonora, Mexico. Trans R Soc Trop Med Hyg. 2018;112:109–14. DOIGoogle Scholar
- Bustamante ME, Varela G. A new rickettsiosis in Mexico. Existence of American spotted fever in the states of Sinaloa and Sonora [in Spanish]. Rev Inst Salubr Enferm Trop. 1943;4:189–211.
- Bustamante ME, Varela G. Characteristics of Rocky Mountain spotted fever in Sonora and Sinaloa, Mexico (study of 12 cases and 2 strains) [in Spanish]. Rev Inst Salubr Enferm Trop. 1944;5:129–34.
- Tinoco-Gracia L, Quiroz-Romero H, Quintero-Martínez MT, Rentería-Evangelista TB, González-Medina Y, Barreras-Serrano A, et al. Prevalence of Rhipicephalus sanguineus ticks on dogs in a region on the Mexico-USA border. Vet Rec. 2009;164:59–61. DOIGoogle Scholar
- Paddock CD. Perspectives on the laboratory diagnosis of rickettsial diseases in the 21st century. Acta Med Costarric. 2013;55:13–24.
- Stewart AG, Stewart AGA. An update on the laboratory diagnosis of Rickettsia spp. infection. Pathogens. 2021;10:1319. DOIGoogle Scholar
- Regan JJ, Traeger MS, Humpherys D, Mahoney DL, Martinez M, Emerson GL, et al. Risk factors for fatal outcome from Rocky Mountain spotted fever in a highly endemic area—Arizona, 2002–2011. Clin Infect Dis. 2015;60:1659–66. DOIGoogle Scholar
- Buonacera A, Stancanelli B, Colaci M, Malatino L. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23:3636. DOIGoogle Scholar
- Jiang J, Liu R, Yu X, Yang R, Xu H, Mao Z, et al. The neutrophil-lymphocyte count ratio as a diagnostic marker for bacteraemia: a systematic review and meta-analysis. Am J Emerg Med. 2019;37:1482–9. DOIGoogle Scholar
- Paddock CD, Alvarez-Hernandez G. Rickettsia rickettsii (Rocky Mountain spotted fever). In: Long SS, Long SS, Prober GC, Fischer M, Kimberlin D, editors. Principles and practice of pediatric infectious diseases, sixth edition. Philadelphia: Elsevier; 2023. p. 971–975.
- Centers for Disease Control and Prevention. National Notifiable Diseases Surveillance System. Spotted fever rickettsiosis (including Rocky Mountain spotted fever) (SFR, including RMSF) 2020 case definition [cited 2025 Nov 24]. https://ndc.services.cdc.gov/case-definitions/spotted-fever-rickettsiosis-2020
Figures
Tables
Cite This Article1Preliminary results from this study were presented at the Southeastern Pediatric Research Conference; June 6, 2025; Atlanta, Georgia, USA; and at the American Society of Tropical Medicine and Hygiene Conference; November 10, 2025; Toronto, Ontario, Canada.
2These senior authors contributed equally to this article.
Table of Contents – Volume 32, Number 2—February 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Kristy O. Murray, Department of Pediatrics, Emory University School of Medicine, and Children’s Healthcare of Atlanta, 2015 Uppergate Dr, Atlanta, GA 30322, USA
Top