Volume 32, Number 6—June 2026
Research Letter
Neisseria gonorrhoeae Sequence Type 16676 in Disseminated Infections, Minnesota, USA, 2025
Cite This Article
Citation for Media
Abstract
We summarize an outbreak investigation of Neisseria gonorrhoeae sequence type 16676 associated with disseminated gonococcal infections in Minnesota, USA, in 2025. This strain emerged rapidly, carried a plasmid with a tetracycline resistance gene, and encoded a porB1a allele. Prospective genomic surveillance enabled detection and epidemiologic investigation of this outbreak.
The sexually transmitted pathogen Neisseria gonorrhoeae can circulate from mucosal tissue at sites of exposure to other locations in the body, causing disseminated gonococcal infection (DGI) (1). In 2024, the Minnesota (USA) Department of Health initiated whole-genome sequencing (WGS) analysis of isolates from all DGI cases in the state (2). This article expands upon our previous study from 2024 (2).
In 2025, cases of DGI in Minnesota continued to occur at an elevated incidence rate compared with the 2020–2023 baseline. Minnesota state reporting rules require N. gonorrhoeae specimens from normally sterile sites to be submitted to the state public health laboratory. Analysis of those cases and linked specimens is considered enhanced surveillance and therefore deemed exempt from Institutional Review Board approval.
Figure 1

Figure 1. Midpoint-rooted phylogenetic tree constructed from an alignment of 1,626 core genes shared by 50 genomes of Neisseria gonorrhoeae isolates from study of outbreak of N. gonorrhoeaeST16676...
We performed WGS using the Illumina MiSeq, NextSeq, or MiSeq i100 platforms (https://www.illumina.com) and performed molecular epidemiologic analyses as previously described (2). Our genomic investigation showed that a new multilocus sequence type (ST), ST16676, emerged during the summer of 2025 (3,4). During June–September 2025, we sequenced 14 isolates from DGI cases whose genomes were assigned to ST16676. All 14 genomes encoded a porB1a allele, the tetracycline resistance gene tet(M), the extended spectrum β-lactamase gene blaTEM, a Type XIV nonmosaic penA allele, and a gonococcal genetic island sequence (Figure 1; Appendix Table, Figure 1) (3–6). Those genomes did not match any documented N. gonorrhoeae sequence type by antimicrobial resistance profiles (5). Long-read sequencing (Oxford Nanopore Technologies, https://nanoporetech.com) of 4 ST16676 isolates consistently resolved the acquired tet(M) and blaTEM genes on separate plasmid sequences of 42kb and 5.6kb and the porB1a allele on the bacterial chromosome.
Figure 2
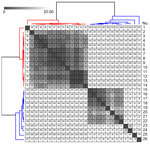
Figure 2. Reference-based pairwise single-nucleotide polymorphism (SNP) matrix of 26 Neisseria gonorrhoeae sequence type 16676 infections from study of outbreak of N. gonorrhoeaesequence type 16676 among disseminated infections,...
In October 2025, we performed a global comparison of those genomes to others in the National Center for Biotechnology Information Pathogen Detection database (https://www.ncbi.nlm.nih.gov/pathogens). That comparison grouped the genomes into a cluster (PDS000214546.4) with 12 other genomes (Appendix Figure 2). Analysis of those 26 genomes using the Dryad version 3.0 pipeline showed that the Minnesota DGI genomes ranged in genetic similarity to each other by 0–62 (median 6) single-nucleotide polymorphisms (SNPs) and to the other 12 genomes by 215–320 (median 248) SNPs (Figure 2) (Dryad, https://github.com/wslh-bio/dryad). An iterative time-scaled phylodynamic analysis of those genomes showed that 28 of 32 iterations converged at early May 2025, weeks before the first case-patient sought care, as an estimated time of a most recent common ancestor for all 14 Minnesota genomes (Appendix) (7).
Epidemiologists completed investigations of ST16676 DGI cases on the basis of findings from genomic surveillance. Of the 13 ST16676-infected case-patients interviewed, 12 (92.3%) resided within the Minneapolis-St. Paul-Bloomington metropolitan area; 11 (84.6%) were male and 2 (15.5%) female, and 9 (69.2%) were 15–44 years of age. Seven (53.8%) case-patients reported anonymous sexual encounters with multiple partners, 3 (23.1%) of whom reported substance use while doing so. Two (15.4%) reported having used doxycycline postexposure prophylaxis. Nine (69.2%) case-patients reported previous sexually transmitted infections; 4 (44.4%) reported gonorrhea and 5 (55.5%) reported HIV. Epidemiologic investigation confirmed a direct link between 2 cases whose isolates’ genomes were genetically identical at 0 SNPs. The 14th case-patient, who refused interviews, had an isolate that was identical at 0 SNPs to the 2 directly linked isolates, lived in an adjacent state, and received care for the infection in Minnesota.
Antimicrobial susceptibility test results were available in medical records of 10 (71.4%) of the 14 ST16676-infected patients. Consistent with results from N. gonorrhoeae sequence type by antimicrobial resistance and AMRFinderPlus analyses (5,6), all 10 isolates showed phenotypic resistance to tetracycline and ciprofloxacin and phenotypic susceptibility to ceftriaxone.
Prospective WGS detected the emergence of a tetracycline-resistant strain of N. gonorrhoeae that replaced the predominant DGI-associated strain from the previous year. The sudden emergence of a DGI-associated strain that carries both a porB1a allele (8) and a tetracycline resistance gene on a mobilizable plasmid poses epidemiologic concern, given the use of doxycycline postexposure prophylaxis to reduce potential illness and subsequent transmission risk of gonorrhea (9). In addition, the presence of 2 antimicrobial resistance genes on separately mobilizable plasmids highlights the importance of monitoring horizontal gene transfer in genomic surveillance of N. gonorrhoeae.
Our findings highlight the importance of DGI surveillance and the value of genomic surveillance for sexually transmitted infections. Prompt case investigations spurred by genomic analysis enabled epidemiologists to identify a direct link between DGI cases and notify a neighboring state health agency of transmission. Phylodynamic approaches also yielded insights into rates at which DGI-associated strains can emerge by estimating a timeline of weeks to months between the estimated time of a most recent common ancestor of a strain and the time at which infected case-patients sought care at healthcare facilities. Continuing prospective genomic surveillance, including performing large-scale studies of the evolution of DGI-causing N. gonorrhoeae strains, will help the field more thoroughly understand and intervene against this public health threat.
This article was preprinted at https://doi.org/10.64898/2026.01.09.26343522.
Mr. Evans is a genomic epidemiologist with the Minnesota Department of Health. His work focuses on developing, implementing, and optimizing the use of microbial genomics for pathogen surveillance and outbreak intervention.
Acknowledgments
We thank Amber Poppe for her support of this epidemiological investigation. We also thank Marcie Babcock, Jeffrey Dennis, Hannah Friedlander, Brian Kendrick, Dakota Schneider, and Jennifer Zipprich for their support of STI surveillance in Minnesota. We acknowledge John C. Cartee and Sandeep J. Joseph for conducting nationwide genomic surveillance that contextualized the results of our local investigations. We also thank the National Center for Biotechnology Information Pathogen Detection team, as well as all healthcare providers in Minnesota and Wisconsin who provided clinical care to patients with disseminated gonococcal infection and reported cases to the Minnesota Department of Health.
Sequencing reads and genome assemblies for the N. gonorrhoeae genomes sequenced for this study are publicly available at the National Center for Biotechnology Information (BioProject no. PRJNA1204341).
Funding for this investigation was provided through the following Centers for Disease Control and Prevention–funded grants: Strengthening STD Prevention and Control for Health Departments Award (grant no. NH25PS005172), Emerging Infections Program (grant no. NU50CK000648), Epidemiology and Laboratory Capacity (grant nos. NU51CK000361 and NU50CK000508), and Pathogen Genomics Centers of Excellence (grant no. NU50CK000628). The findings do not necessarily reflect the official opinions of the agencies that funded this work.
References
- Weston EJ, Heidenga BL, Farley MM, Tunali A, D’Angelo MT, Moore A, et al. Surveillance for disseminated gonococcal infections, active bacterial core surveillance (ABCs)—United States, 2015–2019. Clin Infect Dis. 2022;75:953–8. DOIPubMedGoogle Scholar
- Evans D, Friedlander H, Bo-Subait K, Dennis J, Kaiyalethe J, Craft B, et al. Genomic investigation of disseminated gonococcal infections, Minnesota, USA, 2024. Emerg Infect Dis. 2025;31:2003–7. DOIPubMedGoogle Scholar
- Jolley KA, Bray JE, Maiden MCJ. Open-access bacterial population genomics: BIGSdb software, the PubMLST.org website and their applications. Wellcome Open Res. 2018;3:124. DOIPubMedGoogle Scholar
- Maiden MC, Bygraves JA, Feil E, Morelli G, Russell JE, Urwin R, et al. Multilocus sequence typing: a portable approach to the identification of clones within populations of pathogenic microorganisms. Proc Natl Acad Sci U S A. 1998;95:3140–5. DOIPubMedGoogle Scholar
- Demczuk W, Sidhu S, Unemo M, Whiley DM, Allen VG, Dillon JR, et al. Neisseria gonorrhoeae sequence typing for antimicrobial resistance, a novel antimicrobial resistance multilocus typing scheme for tracking global dissemination of N. gonorrhoeae strains. J Clin Microbiol. 2017;55:1454–68. DOIPubMedGoogle Scholar
- Feldgarden M, Brover V, Gonzalez-Escalona N, Frye JG, Haendiges J, Haft DH, et al. AMRFinderPlus and the Reference Gene Catalog facilitate examination of the genomic links among antimicrobial resistance, stress response, and virulence. Sci Rep. 2021;11:12728. DOIPubMedGoogle Scholar
- Sagulenko P, Puller V, Neher RA. TreeTime: maximum-likelihood phylodynamic analysis. Virus Evol. 2018;4:
vex042 . DOIPubMedGoogle Scholar - Welch G, Reed GW, Rice PA, Ram S. A meta-analysis to quantify the risk of disseminated gonococcal infection with porin B serotype. Open Forum Infect Dis. 2024;11:
ofae389 .PubMedGoogle Scholar - Berçot B, Assoumou L, Caméléna F, Voitichouk C, Mérimèche M, Ouattara M, et al. Antimicrobial drug-resistant Neisseria gonorrhoeae (GC) infections in men using doxycycline postexposure prophylaxis. A substudy of the ANRS 174 DOXYVAC trial. Clin Infect Dis. 2025;
ciaf591 ; [Epub ahead of print].PubMedGoogle Scholar
Figures
Cite This ArticleOriginal Publication Date: May 19, 2026
Table of Contents – Volume 32, Number 6—June 2026
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Daniel Evans, Minnesota Department of Health—Public Health Laboratory, 601 Robert St N, St. Paul, MN 55101, USA
Top