Volume 8, Number 11—November 2002
THEME ISSUE
Tuberculosis Genotyping
Tuberculosis Genotyping Network, United States
Use of DNA Fingerprinting To Investigate a Multiyear, Multistate Tuberculosis Outbreak
Cite This Article
Citation for Media
Abstract
In 1998–1999, the Baltimore TB control program detected a cluster of 21 tuberculosis (TB) cases. Patients reported frequent travel to various East Coast cities. An investigation was conducted to determine whether transmission of the same Mycobacterium tuberculosis strain was occurring in these other localities. A collaborative investigation among federal, state, and local TB controllers included TB record reviews, interviews of patients, and restriction fragment length polymorphism (RFLP) analysis of selected M. tuberculosis isolates from diagnosed TB patients in several cities in 1996–2001. A national TB genotyping database was searched for RFLP patterns that matched the outbreak pattern. Eighteen additional outbreak-related cases were detected outside of Baltimore—the earliest diagnosed in New Jersey in 1996, and the most recent in New York City in late 2001. The outbreak demonstrates the need for strategies to detect links among patients diagnosed with TB across multiple TB control jurisdictions.
Tuberculosis (TB) rates have been declining in the United States since 1993; they reached a low of 5.6 cases per 100,000 population in 2001 (1). To continue this downward trend and eventually achieve the national goal of TB elimination (<1 case per 1 million population per year), ongoing transmission of Mycobacterium tuberculosis in social networks needs to be detected earlier (2). When transmission patterns include interstate travel, the epidemiologic connections among TB patients from different localities are often unrecognized, thus inhibiting the ability of local TB controllers to identify a widespread outbreak. New methods that overcome this logistical difficulty will facilitate TB control in this era of increased mobility among difficult-to-reach populations.
Genetic typing methods to differentiate strains of M. tuberculosis are useful in identifying disease clusters resulting from recent transmission (3–5). Beginning in August 1999, the Centers for Disease Control and Prevention (CDC) facilitated a cross-jurisdictional investigation of a TB outbreak first recognized in Baltimore, Maryland, and described by Sterling et al. (6). We present results of this extended investigation that uncovered 18 additional outbreak cases after the original 21 were described. Most of these additional patients lived outside the state of Maryland. The outbreak demonstrates the value of a system that allows M. tuberculosis strains to be compared across TB control jurisdictions, particularly in situations where unique social and cultural circumstances hinder conventional approaches to contact investigations and control efforts.
Baltimore Outbreak Profile
Between June 1998 and June 1999, TB was diagnosed in 13 young-adult, U.S.-born African-Americans in Baltimore, Maryland; 8 (62%) were HIV positive. Their M. tuberculosis isolates shared a common 11-band DNA fingerprint (6). Upon a review of the National Tuberculosis Genotyping and Surveillance Network database (7), two additional Maryland patients were found to have isolates matching this cluster. Baltimore investigators also suspected that two TB patients in New York City were part of this cluster, a fact that was later verified through genotyping of the patients’ isolates. Among these patients with culture-confirmed TB (age range 18–35 years), all but one were associated with the transgender community (6). The transgender persons were members of a “house,” a social organization of young-adult transgender persons. House members do not necessarily reside together but regularly engage in dance and dressing competitions known as “balls.” A network of several dozen houses exists on the U.S. East Coast (McElroy, unpub. data). Owing to house members’ reported travel patterns, Baltimore investigators suspected that transmission of this same 11-band strain was occurring in other areas, particularly New York City, New Jersey, Atlanta, Boston, Philadelphia, San Francisco, and Washington, D.C. In August 1999, CDC epidemiologists initiated an interstate investigation of this outbreak.
Genetic Typing
Restriction fragment length polymorphism (RFLP) analysis (DNA fingerprinting) of M. tuberculosis isolates was performed according to standard methods (8). RFLP patterns were considered to match if the patterns were identical or differed by the addition or subtraction of a single band.
Search of National Tuberculosis Genotyping Network Database
An image of the 11-band Baltimore outbreak strain was compared to RFLP images in the TB genotyping network database at CDC. This database contains >6,000 unique fingerprint images collected in the period January 1996–December 2000 from Arkansas, Maryland, Massachusetts, Michigan, New Jersey, five counties in Texas, and the San Francisco Bay area. Images were analyzed with BioImage Whole Band Analyzer software, version 3.4 (Genomic Solutions, Inc, Ann Arbor, MI). Pairs of patterns were compared for matching bands by using a deviation of ±2.5% for molecular weight of each band. Patterns were clustered by using the unweighted pair group method with arithmetic averages (UPGMA/Average) linkage. All matches were verified by visual comparison.
New York City Investigation
Before 2001, New York City did not routinely perform RFLP analysis. RFLP was retrospectively performed on isolates obtained from 1998 to 2000 from TB patients with demographic characteristics similar to those of the Baltimore outbreak patients (9). After New York City patients associated with the outbreak were identified, their addresses were cross-matched with the entire New York City TB registry. RFLP analysis was performed on isolates from any patient with a street address matching an outbreak-related case. Beginning in January 2001, RFLP analysis was routinely performed on isolates from all TB patients diagnosed in New York City.
Other City Investigations
In Atlanta and Philadelphia, TB charts of patients fitting the outbreak profile were reviewed, and RFLP analyses were performed on isolates from patients strongly suspected of being part of the outbreak. All isolates from Boston and San Francisco are included in the National Tuberculosis Genotyping and Surveillance Network database, which was searched for matches. San Francisco, although part of the genotyping network, also had a database of additional images from cases preceding 1996. Health authorities in Washington, D.C., did not participate in this investigation.
Epidemiologic Investigations
A member of the outbreak investigation team contacted patients with isolates found to have an RFLP pattern matching the outbreak strain. Patients or next-of-kin (for deceased persons) were interviewed, either by telephone or in person. A questionnaire was used to assess regular travel destinations, ball attendance, cross-dressing behaviors, and membership in a house.
Figure
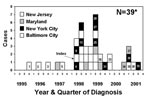
Figure. Epidemic curve representing 38 tuberculosis patients associated with an outbreak involving the cities of Baltimore and New York and the states of Maryland and New Jersey, 1995−2001. *Numbered boxes represent additional...
As of December 31, 2001, this TB outbreak included 39 patients (36 with culture-confirmed disease) from New Jersey, Maryland, New York City, and Baltimore (Figure). RFLP analysis of the 36 M. tuberculosis isolates indicated a matching 11-band pattern in 34 isolates; 2 isolates shared the same 11-band pattern plus 1 additional band. All isolates were susceptible to first-line anti-TB medications. Clinical and demographic characteristics are presented in Tables 1 and 2, respectively.
New Jersey
The initial search of the 6,000 RFLP images in the network database in August 1999 yielded two New Jersey isolates that matched the outbreak strain. The earliest matching RFLP pattern came from an isolate cultured in November 1996 from a 17-year-old woman (patient 3), the sister of a culture-negative 7-year-old girl (patient 2) with clinical TB that had been diagnosed earlier that year (Figure). The second match was an isolate from a 33-year-old woman whose TB was diagnosed in 1997 (patient 5). These three patients were contacts from either the household (patients 2 and 3) or workplace (patient 5) of a 24-year-old man (patient 1) in whom pulmonary TB was diagnosed in 1995, one year preceding initiation of the genotyping network in New Jersey. Thus, although no isolate was available from case-patient 1 at the time of the 1999–2000 outbreak investigation, he was epidemiologically linked to this outbreak. This patient reported a history of frequent travel to New York, Baltimore, Philadelphia, and Atlanta to attend and compete in balls but denied ever being a member of a house and had no identified link to any outbreak cases. The most recent New Jersey patient associated with this outbreak was a transsexual who had undergone male-to-female postoperative surgery (patient 30); her case of TB had been diagnosed in September 1999, and she died in early 2000. As of this writing (mid-2002), no other New Jersey isolates match the outbreak strain.
New York City
RFLP analyses performed on 235 isolates from selected patients diagnosed in 1998–2000 identified seven additional patients (nos. 6, 8, 13, 25, 27, 31, and 36) not previously recognized as being associated with each other or any outbreak case-patients in Baltimore. Interviews indicated that all patients but one (patient 31) were part of the same transgender network described in the Baltimore outbreak. TB was diagnosed in patient 6 in the same month as the case in the Baltimore index patient. The address cross-match identified patient 31, a 1-year old boy who resided in an apartment across the hallway from patient 28. The child’s isolate had an RFLP pattern matching the outbreak strain. Neither patient’s list of identified contacts included the other patient’s name.
Since January 2001, two additional outbreak cases have been identified from New York City after implementation of universal RFLP analysis for isolates obtained from all TB patients in that city. Patient 36 is the only Latino thus far associated with the outbreak. The latest known patient associated with this outbreak (patient 39) was an HIV-coinfected transsexual who had not undergone sex change surgery; plural TB was diagnosed in September 2001.
Maryland
Two additional cases were diagnosed in Maryland after the original report, both in persons from counties bordering Baltimore City. A 42-year-old man with meningeal TB (patient 34) died before he could be interviewed regarding his association with other persons in the outbreak, and his family has not cooperated with this investigation. A 46-year-old woman (patient 37) relocated from New Jersey to Maryland just before her TB diagnosis. The RFLP pattern of her isolate matched the outbreak strain, and subsequent interviews (corroborated by employment records) revealed that in 1996 she worked as a custodian at the same county hospital in New Jersey where patient 1 was hospitalized for TB, on the same floor.
Baltimore
To date, TB was been diagnosed in three additional patients with isolates matching the outbreak strain in Baltimore since the first report (6). Both male patients (patients 33 and 38) were associated with the transgender network. One female patient (patient 35) had contact with a son of the nightclub owner whose club was frequented by most outbreak patients.
Other Sites
RFLP analysis performed on available isolates from patients fitting the outbreak profile in Atlanta (n=26) and Philadelphia (n=3) found that none matched the outbreak strain. RFLP patterns of four San Francisco isolates from the pre-1996 database closely resembled the outbreak strain. These isolates were retyped in 2001 but did not match the outbreak strain. No isolates from Massachusetts or other TB genotyping network sites matched the outbreak strain.
Ongoing transmission of M. tuberculosis in this outbreak occurred in multiple jurisdictions for at least 4 years (1996–1999). Early recognition of this outbreak by the City of Baltimore TB Control Program staff and their suspicion of a larger outbreak network beyond that city were critical to the initiation of the multistate investigation. The transient nature of the outbreak’s social network within Baltimore and the members’ propensity for frequent travel and shared accommodations in other cities created an opportunity for extensive transmission of M. tuberculosis. Subsequently, the high prevalence of HIV coinfection within this population led to an increased likelihood of progression from latent TB infection to TB disease (10). Through the detection of isolates with matching RFLP patterns, followed by interviews with patients regarding their travel to and participation in transgender social events, TB controllers were able to plan and implement specific interventions for this population. Outbreak-associated cases continue to be detected. Continued transmission of this strain is possible, given that pleural disease was diagnosed in a 29-year-old HIV-coinfected patient in September 2001.
DNA fingerprinting of M. tuberculosis isolates has proven to be an extremely useful tool for tracking transmission of various genotypes throughout communities. This technology has a demonstrated role in investigations of transmission within facilities such as prisons (11), hospitals (12), other localized settings such as homeless shelters (13), or in individual states (14). However, few studies have used RFLP to uncover outbreak networks across geographic areas this large. The predictive value of RFLP patterns to document recent M. tuberculosis transmission and the relatedness of isolates is often considered stronger in outbreak settings in which links among patients are known (14). This investigation demonstrated that, after a general demographic profile was established among a group of TB patients (e.g., 18- to 35-year-old, HIV-positive, African-American men) from one locality, typing of isolates from other localities allowed investigators to successfully uncover additional matching isolates from patients with characteristics similar to those of the Baltimore cluster. This outbreak demonstrated the value of periodically comparing RFLP fingerprint patterns beyond local jurisdictions to establish whether transmission of a particular strain extends to a broader geographic area. During the second quarter of 1998, four cases with isolates retrospectively matching the outbreak strain were diagnosed in Baltimore and New York City. By early 1998, the national TB genotyping network database already included at least three isolates from New Jersey and Maryland that matched the outbreak strain. Earlier recognition of the common sociodemographic links among the initial case-patients in multiple localities might have averted the subsequent cases diagnosed between 1999 and the present.
Casual transmission of M. tuberculosis is defined as transmission from an infectious TB patient to persons who are not household, work, school, or close contacts (15). This outbreak included three patients with isolates matching the RFLP pattern of the outbreak strain but with no identified epidemiologic link to other cases, despite extensive investigation. One should be cautious about viewing cases with no clear epidemiologic link as evidence of casual transmission. These patients’ denial of any association with the outbreak network may be a consequence of the secretive nature of some transgender persons, who are often ostracized by society. Some of the male outbreak patients appeared as women only on occasion, and otherwise assimilated into their jobs or schools as men. Many of the transgender patients also engaged in commercial sex work, another potential source of exposure for patients with no identifiable ties to other outbreak patients.
The detection of matching RFLP patterns alone was insufficient to allow investigators to fully characterize the social network in which transmission was occurring. As RFLP analysis of M. tuberculosis isolates is performed on a routine basis in large urban areas (e.g., New York City), case-clusters will continue to emerge. As this happens, TB controllers will be expected to direct interventions toward these apparent clusters. Our investigation confirmed that simply detecting a disease cluster, without describing and understanding the social milieu supporting transmission, can lead to incomplete and inefficient TB control. Cutting-edge molecular tools can be enhanced by equally novel epidemiologic approaches. The role of alternative epidemiologic methods such as network analysis, used in tandem with DNA fingerprint analysis, warrants further investigation (16,17).
Dr. McElroy is an epidemiologist with the Outbreak Investigation Section (OIS) in the Division of Tuberculosis Elimination, Centers for Disease Control and Prevention. OIS responds to requests from state and local health departments for on-site epidemiologic assistance when ongoing transmission of Mycobacterium tuberculosis is suspected. Dr. McElroy is also project officer for a study examining the usefulness of network analysis as a tool for tuberculosis control.
Acknowledgments
We thank the following persons, who provided epidemiologic or laboratory support during various stages of this investigation during 1999–2001: Athalia Christie, Shama Ahuja, Monica Lathan, Sarah Bur, Nancy Baruch, Leonard Mukasa, Deidre Thompson, Richard Stanley, Azalea Madison, George Brubach, Dawn Tuckey, Jacqueline Elliot, Patrick Brennan, Antonio Paz, Beverly DeVoe, Henry Blumberg, and Diane Stemler. Alejandro Marcel provided expert advice and educational materials regarding transgender health issues.
Portions of this work were supported by Centers for Disease Control and Prevention cooperative agreement funds for the National Tuberculosis Genotyping and Surveillance Network.
References
- Centers for Disease Control and Prevention. Reported tuberculosis in the United States. 2000. Atlanta: U.S. Department of Health and Human Services; 2002.
- Institute of Medicine. Ending neglect: the elimination of tuberculosis in the United States. Washington: National Academy Press; 2000.
- Small PM, Hopewell PC, Singh SP, Paz A, Parsonnet J, Ruston DC, The epidemiology of tuberculosis in San Francisco: a population-based study using conventional and molecular methods. N Engl J Med. 1994;330:1703–9. DOIPubMedGoogle Scholar
- Valway SE, Sanchez MPC, Shinnick TF, An outbreak involving extensive transmission of a virulent strain of Mycobacterium tuberculosis. N Engl J Med. 1998;338:633–9. DOIPubMedGoogle Scholar
- Agerton TB, Valway SE, Blinkhorn RJ, Orme I, Agerton T, Hoy D, Spread of strain W, a highly drug-resistant strain of Mycobacterium tuberculosis, across the United States. Clin Infect Dis. 1999;29:85–92. DOIPubMedGoogle Scholar
- Sterling TR, Thompson D, Stanley RL, McElroy PD, Madison A, Moore K, A multi-state outbreak of tuberculosis among members of a highly mobile social network: implications for tuberculosis elimination. Int J Tuberc Lung Dis. 2000;4:1066–73.PubMedGoogle Scholar
- Hale YM, Pfyffer GE, Salfinger M. Laboratory diagnosis of mycobacterial infections: new tools and lessons learned. Clin Infect Dis. 2001;33:834–46. DOIPubMedGoogle Scholar
- van Embden JDA, Cave MD, Crawford JT, Dale JW, Eisenach KD, Gicquel B, Strain identification of Mycobacterium tuberculosis by DNA fingerprinting: recommendations for a standardized methodology. J Clin Microbiol. 1993;31:406–9.PubMedGoogle Scholar
- Centers for Disease Control and Prevention. HIV-related tuberculosis in a transgender network—Baltimore, Maryland and New York City area, 1998–2000. MMWR Morb Mortal Wkly Rep. 2001;49:317–20.
- Selwyn PA, Sckell BM, Alcabes P, Friedland GH, Klein RS, Schoenbaum EE. High risk of active tuberculosis in HIV-infected drug users with cutaneous anergy. JAMA. 1992;268:504–9. DOIPubMedGoogle Scholar
- March F, Coll P, Guerrero RA, Busquets E, Cayla JA, Prats G, Predictors of tuberculosis transmission in prisons: an analysis using conventional and molecular methods. AIDS. 2000;14:525–35. DOIPubMedGoogle Scholar
- Hennessey KA, Schulte JM, Valway SE, Joglar OT, Rios N, Sheppard JD, Using DNA fingerprinting to detect transmission of Mycobacterium tuberculosis among AIDS patients in two health-care facilitites in Puerto Rico. South Med J. 2000;93:777–82.PubMedGoogle Scholar
- Curtis AB, Ridzon R, Novick LF, Driscoll J, Blair D, Oxtoby M, Analysis of Mycobacterium tuberculosis transmission in a homeless shelter outbreak. Int J Tuberc Lung Dis. 2000;4:308–13.PubMedGoogle Scholar
- Braden CR, Templeton GL, Cave MD, Valway S, Onorato IM, Castro KG, Interpretation of restriction fragment length polymorphism analysis of Mycobacterium tuberculosis isolates from a state with a large rural population. J Infect Dis. 1997;175:1446–52. DOIPubMedGoogle Scholar
- Onorato IM. Tuberculosis outbreaks in the United States. Int J Tuberc Lung Dis. 2000;4(Suppl 2):S134–8.PubMedGoogle Scholar
- Klovdahl AS, Graviss EA, Yaganehdoost A, Ross MW, Wanger A, Adams GJ, Networks and tuberculosis: an undetected community outbreak involving public places. Soc Sci Med. 2001;52:681–94. DOIPubMedGoogle Scholar
- Fitzpatrick LK, Hardacker JA, Heirendt W, Agerton T, Streicher A, Melnyk H, A preventable outbreak of tuberculosis investigated through an intricate social network. Clin Infect Dis. 2001;33:1801–6. DOIPubMedGoogle Scholar
Figure
Tables
Cite This Article1 PDM, TRS, CRD, BK, CLW, WAC, DXH, KLS, and RR were involved in the conception and design of various phases (epidemiologic and laboratory methods) of this investigation. All coauthors were responsible for collection of either epidemiologic or molecular genotyping data. Analysis and interpretation of the data were primarily performed by PDM, TRS, and RR. All coauthors participated in preparation and critical review of the manuscript.
Table of Contents – Volume 8, Number 11—November 2002
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Peter D. McElroy, Division of Tuberculosis Elimination, Mailstop E10, Centers for Disease Control and Prevention, 1600 Clifton Rd, NE, Atlanta, GA 30333; fax: 404-639-8959;
Top