Volume 9, Number 11—November 2003
Perspective
Risks and Benefits of Preexposure and Postexposure Smallpox Vaccination1
Figure 3
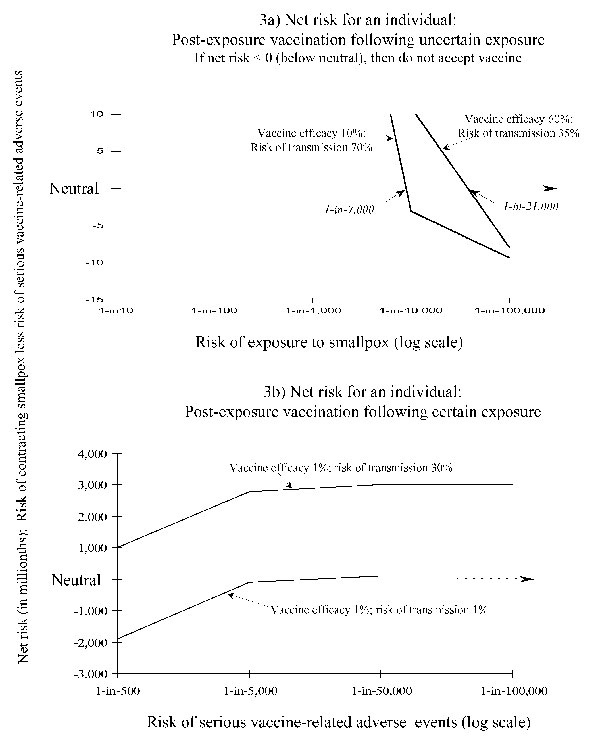
Figure 3. Risk-benefit analyses for persons considering postexposure smallpox vaccination: two scenarios. If the net risk is >0 (above neutral), then the person will accept postexposure vaccination. In the net risk is <0 (below neutral), then the person would not accept postexposure vaccination. Part a shows the net risk for postexposure smallpox vaccination for a person who has been exposed to somebody who may or may not have smallpox (i.e., the exposure is uncertain). Threshold values of risk for exposure to smallpox, when net risk = 0 (neutral), are rounded to the nearest 1,000. Part b shows the net risk for an individual person who has been exposed to a definite smallpox case (see text for further details).
1This article presents further ethodologic details and results of a study presented at a workshop entitled “Scientific and policy considerations in developing smallpox vaccination options,” Washington, DC, 2002 (1).
2Assume that only a single metropolitan population of 9 million is at risk from an initial attack, and the initial attack results in 1,000 cases before discovery. For a person in that population, the risk for death from smallpox is approximately 33 times greater than the risk for death from the smallpox vaccine [smallpox risk for death/vaccine-related risk for death = (1,000 cases/ 9 million x 0.3)/0.000001]. For a person in a population of 280 million, the risk of dying from smallpox in the initial 1,000 cases is approximately equal to the risk for death from the vaccine.
3In data reported by Rao from Madras, India (Figures 17/1 and 17/3 [23]), among the unvaccinated, approximately 80% of all cases of smallpox occurred in children <10 years of age. A distinct shift in age of the case-patients occurred among the vaccinated, with <10% of cases occurring in children <10 years of age, 19% of cases occurring in children 10–19 years, and 46% of cases occurring in persons 20–30 years of age. Rao did not report at what age most of those vaccinated received vaccine (a likely hypothesis would be before 2 years of age). Further complicating the analysis of such data is the fact that many persons in Madras received more than one smallpox vaccination (Figure 17/5, [23]). A similar age-shift in occurrence of cases among the vaccinated can be discerned from the data reported by Hanna (24) from Liverpool, England, in 1902–03. The data from both Rao (23) and Hanna (26) further indicate that even a 20-year-old vaccination may reduce the severity of disease. The risk for death is markedly reduced 20–30 years postvaccination (23,26,27).
4In addition to the estimates quoted in the main text, Rao et al. (39) found that successful postexposure vaccination reduced, on average, the rate of smallpox among contacts by approximately 38% (from 48% among unvaccinated to 30% among postexposure vaccinees). Dixon (40) reported that in a group of 59 contacts under 5 years of age “. . . approximately half of those who had a successful vaccination after contact developed disease.” The wide variations in reports of the degree of protection afforded by postexposure vaccination are probably due to a number of reasons, including small sample sizes and difficulty in determining when exposure and potential transmission actually took place.