Volume 15, Number 10—October 2009
Research
Mycobacterium tuberculosis Genotype and Case Notification Rates, Rural Vietnam, 2003–2006
Cite This Article
Citation for Media
Abstract
Tuberculosis case notification rates (CNRs) for young adults in Vietnam are increasing. To determine whether this finding could reflect emergence of Mycobacterium tuberculosis Beijing genotype, we studied all new sputum smear–positive pulmonary tuberculosis patients registered for treatment in 3 rural districts in Vietnam during 2003–2006. Beijing strain infections were more frequent in younger patients (15–24 years of age, 53%) than in older patients (31%; p<0.001). The increase in CNRs for youngest patients was larger for disease caused by the Beijing genotype than by other genotypes, but the difference was not significant. For patients 15–24 years of age, 85% of fluctuations in CNRs between years was caused by fluctuations in Beijing genotype infections compared with 53% and 23% in the groups 25–64 and >65 years of age, respectively (p<0.001). These findings suggest that young adults may be responsible for introducing Beijing strains into rural Vietnam.
One third of the world’s population is infected with Mycobacterium tuberculosis, and ≈9 million tuberculosis (TB) cases were diagnosed worldwide in 2006 (1). Introduced in the early 1990s, the directly observed treatment, short-course (DOTS) strategy is an essential component of the Global Stop TB Strategy and regarded as a highly cost-effective method for controlling the TB epidemic (2). In addition, the DOTS strategy has resulted in decreased numbers of TB cases in Peru, parts of the People’s Republic of China, India, and Indonesia (3–6) a few years after those countries met the goals of the World Health Organization (WHO), which are to detect >70% and cure >85% of smear-positive TB cases (7).
Conversely, the DOTS strategy has had a limited effect (no decrease in numbers of TB cases) in other regions, such as the former Soviet Union and sub-Saharan Africa (3,8). In Vietnam, TB case notification rates (CNRs) have not decreased since 1997 when the National TB Control Program reached WHO goals (1,9). This absence of a stable rate decrease reflects a decrease in TB CNRs among middle-age persons, primarily women, which is compensated for by an increase in CNRs in young adults, primarily men (10). Several explanations for this phenomenon have been proposed, including the emerging HIV epidemic (11), rapid urbanization (12), and emergence of the M. tuberculosis Beijing genotype (13). Studies worldwide indicated that the Beijing genotype is widespread and associated with drug resistance (14–20). In Vietnam, a study of isolates from patients located mainly in Ho Chi Minh City showed that the Beijing genotype accounted for 55% of the M. tuberculosis isolates and was associated with young age and drug resistance (21). Another study in Ho Chi Minh City found that this genotype was more frequent among patients with treatment failure or relapse (22). Therefore, emergence of the Beijing genotype, or a higher rate of recurrence of Beijing genotype cases, could explain part of the increase in TB rates among young adults. However, these studies were conducted in large urban areas where rapid urbanization and internal immigration may have confounded these associations. Therefore, we assessed, in a population-based study, the role of the Beijing genotype in the TB epidemic in a rural setting in Vietnam. We studied trends in CNRs of new smear-positive TB cases caused by specific genotypes over time by age and sex, and age-specific variations in genotype distribution over time.
The study was conducted at Pham Ngoc Thach Tuberculosis and Lung Disease Hospital, Ho Chi Minh City, Vietnam, and Tien Giang Provincial Tuberculosis and Lung Disease Hospital, My Tho, Vietnam. The study area consisted of 3 adjacent rural districts in Tien Gang Province, situated in the Mekong River Delta in southern Vietnam. These 3 districts have implemented DOTS strategies since 1994. Each district has a district TB unit that examines sputum smears and treats ambulatory patients with smear-positive results according to the DOTS strategy. HIV testing of TB patients is performed only when HIV infection is suspected on the basis of clinical signs. Details of the study area have been described elsewhere (13).
Eligible for inclusion were all patients >15 years of age who were residents in the study area and who had registered for treatment of smear-positive pulmonary TB from January 1, 2003, through December 31, 2006, at the participating district TB units or at the provincial TB hospital, and had started treatment for TB <2 weeks earlier. Smear-positive TB was diagnosed by microscopic examination of >2 Ziehl-Neelsen–stained sputum smears following international guidelines (23,24). Eligible patients were included in the study after they provided written informed consent. Scientific and ethical clearance was obtained from the Ethical Health Committee of the Ho Chi Minh City Council. For technical reasons, in 1 of 3 districts, data collection did not start until 2004.
Data Collection and Laboratory Methods
Included patients were asked to submit 2 pretreatment sputum specimens for Mycobacterium culture. Specimens were refrigerated and transported to the Mycobacterial Reference Laboratory in Ho Chi Minh City within 72 hours. At the reference laboratory, sputum specimens were decontaminated and liquefied with 1%
Notification data for new patients with smear-positive results, by age and sex, during 1997–2006 were obtained from routine reports of the district TB units in the study site. Sex- and age-specific population denominators were interpolated and extrapolated from 1999 and 2004 census data; standard exponential population growth was assumed.
Definitions
Figure 1
Figure 1. Typical spacer patterns of the Mycobacterium tuberculosis spoligotypes most frequently isolated from patients with smear-positive pulmonary tuberculosis, Vietnam, 2003–2006. EAI5 and EAI4 are East African–Indian genotypes.
A new case of new smear-positive TB was defined as a case in a patient who had never had treatment for TB or who had taken drugs for treatment of TB for <1 month (7). The Beijing genotype was defined as any isolate without direct repeat spacers 1–34 and with >3 spacers 35–43 by spoligotyping (26). Other genotypes were defined as described by Brudey et al. (27), including the East-African-Indian Vietnam genotype (EAI-VNM), which belongs to the EAI genotype family of M. tuberculosis and is considered the most common genotype in Vietnam (21,27) (Figure 1).
Data Management and Statistical Analyses
Data were entered into EpiInfo version 6.04 (Centers for Disease Control and Prevention, Atlanta, GA, USA). A 20% random sample was double-entered and discrepancies were checked against raw data. Discrepancies were found in <0.5% of the records and <0.1% of the entries. Analyses were performed by using Stata version 8 (StataCorp LP, College Station TX, USA) and Excel 2003 (Microsoft, Redmond, WA, USA). Patients with negative cultures or cultures that grew nontuberculous mycobacteria were excluded from the analyses.
We used the χ2 test for comparison of proportions. Time trends were assessed by using the Cuzick nonparametric test for trends (28). To assess overall trends of CNRs, age- and sex-specific CNRs were standardized by direct standardization using the 1999 census population as the reference and plotted against time. Exponential trend lines were fitted by using the least-squares method. We calculated trends of CNRs for 2003–2006 by sex, age group, and genotype by using Poisson regression. Trends over time by genotype and age group were assessed by testing for interactions between these variables and the variable year in Poisson regression models and by using the likelihood ratio χ2 test for significance testing.
To analyze variation in genotype distribution over time, we first calculated the absolute differences in CNRs between subsequent years and the proportion of these absolute differences for each genotype. Thereafter, averages of these proportions were calculated; to adjust for differences in changes over time, we weighted these averages by absolute variation per year of summed variation for all years. Significance testing was conducted for numbers of cases (i.e., disregarding the population denominator) by χ2 test comparing genotype against combined strata of year and age group. All tests were conducted at the 5% significance level.
Figure 2
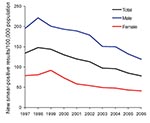
Figure 2. Trends in case notification rates for patients with new smear-positive tuberculosis, by sex, Vietnam, 1997–2006. The annual percentage changes were –4.3% for male patients, –7.7% for female patients, and –5.1% for...
Figure 3
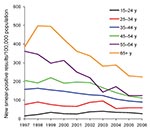
Figure 3. Trends in case notification rates for patients with new smear-positive tuberculosis, by age, Vietnam, 1997–2006. The annual percentage changes were +4.8% for persons 15–24 years of age, –3.3% for those 25–34...
During 1997–2006, CNRs of new smear-positive TB in the study sites decreased by 5.1% per year (95% confidence interval [CI] 4.4%–5.9%), to a lesser extent for men (4.3%, 95% CI 3.4%–5.2%) than for women (7.1%, 95% CI 6.3%–9.1%). Except for patients 15–24 years of age, these decreasing trends were observed for both sexes (Figure 2) and age groups (Figure 3).
During 2003–2006, a total of 2,337 new smear-positive TB patients were registered for treatment in the 3 participating districts; 2,249 (96%) of these patients met inclusion criteria. We excluded 31 patients who did not have data collection forms and 8 other patients whose sputum samples were lost. Patients excluded for this reason did not differ by age or sex from the other patients. A total of 2,210 (94.9%) culture results were available. Of these results, 84 were negative and 29 grew nontuberculous mycobacteria. The remaining 2,097 isolates (89.7%) were genotyped (Table 1).
Of these 2,097 isolates, 682 (32.5%) were of the Beijing genotype, 1,063 (50.7%) were of the Vietnam EAI-VNM genotype, and 353 (16.8%) were of other genotypes. There were no differences in age and sex among the patients from whom the isolates were obtained and subjected to genotyping and all remaining patients registered during the study period. The proportion of isolates with a Beijing genotype was significantly higher for patients 15–24 years of age (52.5%) than for patients of other ages (30.6%; p<0.001). The proportion of isolates with the Vietnam genotype was higher among men and among patients >24 years of age; no differences were found for the other genotypes when combined into 1 group (Table 1). No time trends were evident after stratification of the data by age group or sex.
Because the proportion of genotypes other than Beijing and Vietnam was low and was composed of a heterogeneous group, we limited analyses of CNRs by genotype to the isolates of the Vietnam and Beijing genotypes. The age groups 25–34, 35–44, 45–54, and 55–64 years were grouped together because we found no variation in genotype distribution within these subgroups (Table 1).
During 2003–2006, the overall CNR for new smear-positive TB decreased by an average of –4.3% (95% CI –8.0% to –0.3%) per year. Decreasing trends were also seen for patients 25–64 years of age (–5.1% per year, 95% CI –9.7% to –0.2%) and >65 years of age (–8.0% per year, 95% CI –14.8% to –0.7%). For patients 15–24 years of age, CNRs showed an average annual increase of +5.2% (95% CI –8.4%–20.9%). Rates for women showed an average decrease of –7.9% per year (95% CI –15.2% to –0.2%) and for men, an average decrease of –3.0% per year (95% CI –7.3%–1.6%).
Figure 4

Figure 4. Average annual percentage changes in case notification rates for patients with new smear-positive tuberculosis by age and sex, for the Vietnam genotype (A) and the Beijing genotype (B), Vietnam, 2003–2006. Black...
Overall trends in CNRs were similar for patients infected with the Beijing and with the Vietnam genotypes (decreases of –5.9% and –4.4% per year, respectively) (Figure 4). Decreasing trends were observed for middle-age and elderly persons (–6.3% and –5.0% per year for patients 24–64 years of age and –11.3% and –7.1% per year for patients >65 years of age).
However, for patients 15–24 years of age, CNRs increased for patients infected with either genotype. This increase was higher for those with the Beijing genotype (9.2%) than for those with the Vietnam genotype (2.0%), but this difference was not statistically significant (p = 0.860). This difference could be explained by a divergent trend among women: a 7.3% increase per year for those with the Beijing genotype (95% CI –20.2%–44.3%) versus a –13.6% decrease for those with the Vietnam genotype (95% CI –55.1% to –3.5%, p = 0.360) (Figure 4).
Figure 5

Figure 5. Number of new smear-positive tuberculosis cases, by mycobacterial genotype and patient age, Vietnam, 2003–2006. A), All patients; B) patients 15–24 years of age; C) patients 25–64 years of age; D) patients...
Closer inspection of CNRs during 2003–2006 showed an increase, followed by a decrease, which was consistent across age groups but with different patterns over time (Figure 5). The distribution of genotypes over time differed by age group. After correction for differences in absolute changes between years, the proportion of variation that was caused by the Vietnam genotype was ≈50% for patients >25 years of age but only 3% for patients 15–24 years of age (Figure 5, Table 2). The proportion of variation caused by the Beijing genotype was 85% for patients 15–24 years of age compared with 53% for patients 25–64 years of age and 23% for patients >65 years of age. Differences between the Beijing genotype and remaining genotypes within the youngest and oldest age groups and differences in genotype distribution between the youngest and the oldest age groups were statistically significant (Table 2).
During 1997–2006, CNRs for new smear-positive TB for the study site decreased by 4.3% per year likely due to introduction of the DOTS strategy in 1994. As in other studies in Vietnam (9,10), we found an underlying pattern of increasing CNRs for young adults, which partially compensated for strongly decreasing CNRs for other age groups.
In the study area, where the Beijing genotype is associated with young age and female sex (13), we observed no effect of variations in genotype distribution on the CNRs for all ages and sexes combined. For patients >25 years of age, decreasing trends were observed for the Beijing and Vietnam genotypes. There was also no overall difference in CNRs between men and women. However, for patients 15–24 years of age, an increasing trend for both major genotypes was observed. This trend was stronger for the Beijing genotype than for the Vietnam genotype, although the difference was not significant. This difference was most apparent among women in this age group.
Increases in CNRs among young adults are generally considered to reflect recent increases in transmission (29). Therefore, our findings may suggest that the Vietnam genotype is being replaced by the Beijing genotype at the population level in rural Vietnam. The lack of an association between the genotype and the trend in CNRs could then reflect random error or a too-short observation period (4 years). Larger studies of longer duration may be needed to determine whether such an association exists.
The increase in CNRs of new smear-positive TB for persons 15–24 years of age may also be explained by development of the HIV epidemic. HIV increases the risk for progression of M. tuberculosis infection to TB and probably increases susceptibility to infection (1). In sub-Saharan Africa, 9% of all new TB cases in persons 15–49 years of age were attributable to HIV infection (8). In Ho Chi Minh City, the HIV prevalence among TB patients during 1997–2002 increased exponentially from 1.5% to 9% (11). This increase in CNRs of new smear-positive TB in patients 15–34 years of age was attributable to HIV, although HIV could not explain the lack of an expected decrease. In our study, HIV data for TB patients were not obtained. The estimated prevalence of HIV infection among persons 15–49 years of age in Tien Giang, Vietnam, in 2005 was much lower than in Ho Chi Minh City (0.5%) (30), similar to the national average. The estimated HIV prevalence among TB patients in 30 sentinel provinces was 4.8% in 2004 (D.H. Thanh, Vietnam National Tuberculosis Programme, unpub. data). Thus, it is unlikely that HIV played a role in the observed associations. Furthermore, no association has been found between HIV infection status and isolation of Beijing genotype from pulmonary TB patients elsewhere (31).
However, we have alternative explanations for our results. We found that among young adults, nearly all of the variation in CNRs between the years of collection was attributable to variations in CNRs caused by the Beijing genotype; this variation was less apparent for persons in older age groups. This finding suggests that Beijing strains circulate more abundantly among young adults as a consequence of high transmission rates within this age group. Alternatively, the observed fluctuations in numbers of cases caused by Beijing strains may reflect importation from urban areas. Although we did not collect data from these areas, young adults in Tien Giang often travel (70 km) to Ho Chi Minh City for school or work. This explanation is supported by the following findings: the prevalence of infections with the Beijing genotype among persons with TB in this city was higher than the prevalence of comparable patients in rural districts (13,21) and our earlier result that infections with the Beijing genotype in Tien Giang were more common in patients living along the main road to Ho Chi Minh City (13).
High transmission rates among young adults, particularly in urban areas, may increase emergence of Beijing strain TB infections in Vietnam. Recent data from The Gambia suggest that Beijing strain infections do not show increased secondary attack rates but have shorter incubation periods than other genotypes (32). In settings with high transmission rates, such strains may be preferentially selected. Even if their risk for transmission as such is not increased, their faster progression to TB and infectiousness will give them a selective advantage. This hypothesis may also explain the association between the Beijing genotype and a history of imprisonment (e.g., in the former Soviet Union) (19,33).
To test this hypothesis, more studies of genotype-specific variations in incubation period and variations in genotype between high-transmission and low-transmission settings are needed. Different sublineages of the Beijing genotype may have different pathogenic characteristics (34,35). Data from Vietnam suggest that the more recently evolved typical Beijing strains have a higher propensity to evade immunity from M. bovis BCG vaccination (36). In addition, studies among immigrant populations in the United States, South Africa, and Canada have suggested that the transmission propensity of different genotypes and of different sublineages of the Beijing genotype is dependent on the host population (19,33,35,37–39). Such studies (19,33) should enable analyses of different sublineages of the Beijing genotype and involve non-East Asian populations.
The association of the Beijing genotype with young adults could threaten the effectiveness of the DOTS strategy in Vietnam and elsewhere. However, this possibility is unlikely because in our study, although 25% of the elderly patients were infected by Beijing strains, overall CNRs of TB caused by Beijing strains still decreased. Conversely, associations have been found in some studies, including one in the same study area, between the Beijing genotype and drug resistance, particularly for multidrug-resistant TB (MDR TB) (13,17,18,21,31). Although until 2001 the prevalence of MDR TB among new patients with smear-positive TB in the study area was relatively low and not increasing (40), the effects of genotype-associated risks for increased acquisition or transmission of MDR TB may threaten the effectiveness of long-term TB control.
Our study has several other limitations. First, our data were limited to new patients with smear-positive pulmonary TB and may not be representative of patients with other types of TB, including previously treated patients. In our study area, the Beijing genotype was more prevalent in previously treated patients than in new patients (13), which suggested that a stronger effect of genotype on TB trends might be observed if previously treated patients were included in the analyses. Second, we did not include patients who were treated in the private health sector. We collected no data on the proportion of patients treated in the private sector, but local health authorities estimate the proportion of these patients to be <10%. Third, we did not include children <15 years of age because of ethical constraints and because their number was expected to be small. In Vietnam, children account for no more than 0.2% of notified smear-positive TB cases (National Tuberculosis Program, unpub. data). However, pediatric TB may be underdiagnosed if the only test for diagnosis is microscopic examination of sputum smears.
Our data do not prove or refute that the increase of TB in young adults in rural Vietnam is related to emergence of the Beijing genotype. However, they do suggest that the association between the Beijing genotype and young age reflects importation of Beijing strain infections from urban areas into rural areas. This importation may be linked to or driven by high rates of transmission among young adults.
Dr Buu is an epidemiologist at Pham Ngoc Thach Tuberculosis and Lung Disease Hospital in Ho Chi Minh City, Vietnam. His research interests include the effect of control efforts on the epidemiology of tuberculosis, in particular with regard to HIV infection, drug resistance, and genotype.
Acknowledgments
We thank the staff in Cai Be, Cai Lay, and Chau Thanh for data collection; Frank van Leth and Nico Nagelkerke for discussing statistical issues; Kristin Kremer for technical assistance; and the staff of the Microbiology Department at Pham Ngoc Thach Hospital for processing cultures and genotyping.
This study was supported by the KNCV Tuberculosis Foundation, the Netherlands Committee Netherlands-Vietnam, and the World Health Organization.
References
- World Health Organization. Global tuberculosis control: surveillance, planning, finances. Geneva: The Organization; 2008.
- Baltussen R, Floyd K, Dye C. Cost effectiveness analysis of strategies for tuberculosis control in developing countries. BMJ. 2005;331:1364. DOIPubMedGoogle Scholar
- Subramani R, Santha T, Frieden TR. Active community surveillance of the impact of different tuberculosis measures, Tiruvallur, South India, 1968–2001. Int J Epidemiol. 2007;36:387–93. DOIPubMedGoogle Scholar
- China Tuberculosis Control Collaboration. The effect of tuberculosis control in China. Lancet. 2004;364:417–22. DOIPubMedGoogle Scholar
- Zhang LX, Tu DH, Enarson DA. The impact of directly-observed treatment on the epidemiology of tuberculosis in Beijing. Int J Tuberc Lung Dis. 2000;4:904–10.PubMedGoogle Scholar
- Soemantri S, Senewe FP, Tjandrarini DH, Day R, Basri C, Manissero D, Three-fold reduction in the prevalence of tuberculosis over 25 years in Indonesia. Int J Tuberc Lung Dis. 2007;11:398–404.PubMedGoogle Scholar
- World Health Organization. Treatment of tuberculosis. Guidelines for national programme. Geneva: The Organization; 2003.
- Corbett EL, Marston B, Churchvard GJ, De Cock KM. Tuberculosis in sub-Saharan Africa: opportunities, challenges, and change in the era of antiretroviral treatment. Lancet. 2006;367:926–37. DOIPubMedGoogle Scholar
- Huong NT, Duong BD, Co NV, Quy HT, Tung LB, Broekmans JF, Tuberculosis epidemiology in six provinces of Vietnam after the introduction of the DOTS strategy. Int J Tuberc Lung Dis. 2006;10:963–9.PubMedGoogle Scholar
- Vree M, Buong BD, Sy DN, Co NV, Borgdorff MW, Cobelens FGJ. Tuberculosis trends, Vietnam. Emerg Infect Dis. 2007;13:796–7.PubMedGoogle Scholar
- Tran NB, Houben RM, Hoang TQ, Nguyen TN, Borgdorff MW, Cobelens FG. HIV and tuberculosis in Ho Chi Minh City, Vietnam, 1997–2002. Emerg Infect Dis. 2007;13:1463–9.PubMedGoogle Scholar
- Duc LV, Vree M, Sy DN, Co NV, Borgdorff MW, Cobelens FGJ. Steep increases in tuberculosis notification among young men in the industrialised districts of Danang, Vietnam. Int J Tuberc Lung Dis. 2007;11:567–70.PubMedGoogle Scholar
- Buu TN, Huyen MH, Lan NT, Quy HT, Hen NV, Zignol M, The Beijing genotype is associated with young age and multidrug-resistant tuberculosis in rural Vietnam. Int J Tuberc Lung Dis. 2009;13:900–6.PubMedGoogle Scholar
- Lillebaek T, Andersen AB, Dirksen A, Glynn JR, Kremer K. Mycobacterium tuberculosis Beijing genotype. Emerg Infect Dis. 2003;9:1553–7.PubMedGoogle Scholar
- Jou R, Chiang CY, Huang WL. Distribution of the Beijing family genotypes of M. tuberculosis in Taiwan. J Clin Microbiol. 2005;43:95–100. DOIPubMedGoogle Scholar
- Krüüner A, Hoffner SE, Sillastu H, Danilovits M, Levina K, Svenson SB, Spread of drug-resistant pulmonary tuberculosis in Estonia. J Clin Microbiol. 2001;39:3339–45. DOIPubMedGoogle Scholar
- Bifani PJ, Plikaytis BB, Kapur V, Stockbauer K, Pan X, Lutfey ML, Origin and interstate spread of a New York City multidrug-resistant M. tuberculosis clone family. JAMA. 1996;275:452–7. DOIPubMedGoogle Scholar
- Almeida D, Rodrigues C, Ashavaid TF, Lalvani A, Udwadia ZF, Mehta A. High incidence of the Beijing genotype among multidrug-resistant isolates of M. tuberculosis in a tertiary care center in Mumbai, India. Clin Infect Dis. 2005;40:881–6. DOIPubMedGoogle Scholar
- Balabanova Y, Drobniewski F, Fedorin I, Zakharova S, Nikolayevskyy V, Atun R, The directly observed therapy short course (DOTS) strategy in Samara Oblast, Russian Federation. Respir Res. 2006;7:44. DOIPubMedGoogle Scholar
- Thwaites G, Caws M, Chau TT, D’Sa A, Lan NT, Huyen MN, Relationship between Mycobacterium tuberculosis genotype and the clinical phenotype of pulmonary and meningeal tuberculosis. J Clin Microbiol. 2008;46:1363–8. DOIPubMedGoogle Scholar
- Anh DD, Borgdoff MW, Van LN, Lan NT, van Gorkom T, Kremer K, Mycobacterium tuberculosis Beijing genotype emerging in Vietnam. Emerg Infect Dis. 2000;6:302–5. DOIPubMedGoogle Scholar
- Lan NT, Lien HT, Tung LB, Borgdorff MW, Kremer K, van Soolingen D. Mycobacterium tuberculosis Beijing genotype and risk for treatment failure and relapse, Vietnam. Emerg Infect Dis. 2003;9:1633–5.PubMedGoogle Scholar
- International Union Against Tuberculosis and Lung Disease. Technical guide: sputum examination for tuberculosis direct microscopy in low income countries, 5th ed. Paris: The Union; 2000.
- World Health Organization. Guidelines for surveillance of drug resistance in tuberculosis, 2nd ed. WHO/CDS/TB/2003.313. Geneva: The Organization; 2003.
- Kamerbeek J, Schouls L, Kolk A, van Agterveld M, van Soolingen D, Kuijper S, Simultaneous detection and strain differentiation of Mycobacterium tuberculosis for diagnosis and epidemiology. J Clin Microbiol. 1997;35:907–14.PubMedGoogle Scholar
- Kremer K, Glynn JR, Lillebaek T, Niemann S, Kurepina NE, Kreiswirth BN, Definition of the Beijing/W lineage of M. tuberculosis on the basis of genetic markers. J Clin Microbiol. 2004;42:4040–9. DOIPubMedGoogle Scholar
- Brudey K, Driscoll JR, Rigouts L, Prodinger WM, Gori A, Al-Hajoj SA, Mycobacterium tuberculosis complex genetic diversity: mining the fourth international spoligotyping database (SpolDB4) for classification, population genetics and epidemiology. BMC Microbiol. 2006;6:23. DOIPubMedGoogle Scholar
- Rieder HL. Epidemiology basic of tuberculosis control. 1st ed. Paris: International Union Against Tuberculosis and Lung Disease; 1999.
- HIV/AIDS estimates and projections 2005–2010. Hanoi (Vietnam): Ministry of Health; 2005.
- European Concerted Action on New Generation Genetic Markers and Techniques for the Epidemiology and Control of Tuberculosis. Beijing/W genotype Mycobacterium tuberculosis and drug resistance. Emerg Infect Dis. 2006;12:736–43.PubMedGoogle Scholar
- de Jong BC, Hill PC, Aiken A, Awine T, Antonio M, Adetifa IM, Progression to active tuberculosis, but not transmission, varies by Mycobacterium tuberculosis lineage in The Gambia. J Infect Dis. 2008;198:1037–43. DOIPubMedGoogle Scholar
- Drobniewski F, Balabanova Y, Nikolayevsky V, Ruddy M, Kuznetzov S, Zakharova S, Drug-resistant tuberculosis, clinical virulence, and the dominance of the Beijing strain family in Russia. JAMA. 2005;293:2726–31. DOIPubMedGoogle Scholar
- Toungoussova OS, Sandven P, Mariandyshev AO, Nizovtseva NI, Bjune G, Caugant DA. Spread of drug-resistant Mycobacterium tuberculosis strains of the Beijing genotype in the Archangel Oblast, Russia. J Clin Microbiol. 2002;40:1930–7. DOIPubMedGoogle Scholar
- Hanekom M, van der Spuy GD, Gey van Pittius NC, McEvoy CR, Ndabambi SL, Victor TC, Evidence that the spread of Mycobacterium tuberculosis strains with the Beijing genotype is human population dependent. J Clin Microbiol. 2007;45:2263–6. DOIPubMedGoogle Scholar
- Kremer K, van der Werf MJ, Au BK, Anh DD, Kam KM, van Doorn HR, Vaccine-induced immunity circumvented by typical Mycobacterium tuberculosis Beijing strains. Emerg Infect Dis. 2009;15:335–9. DOIPubMedGoogle Scholar
- Gagneux S, DeRiemer K, Van T, Kato-Maeda M, de Jong BC, Narayanan S, Variable host-pathogen compatibility in Mycobacterium tuberculosis. Proc Natl Acad Sci U S A. 2006;103:2869–73. DOIPubMedGoogle Scholar
- Hanekom M, van der Spuy GD, Streicher E, Ndabambi SL, McEvoy CR, Kidd M, A recently evolved sublineage of the Mycobacterium tuberculosis Beijing strain family is associated with an increased ability to spread and cause disease. J Clin Microbiol. 2007;45:1483–90. DOIPubMedGoogle Scholar
- Reed MB, Pichler VK, McIntosh F, Mattia A, Fallow A, Masala S, Mycobacterium tuberculosis lineages associate with patient country of origin. J Clin Microbiol. 2009;47:1119–28. DOIPubMedGoogle Scholar
- Huong NT, Lan NTN, Cobelens FGJ, Duong BD, Co NV, Bosman MC, Anti-tuberculosis drug resistance in the south of Vietnam: prevalence and trends. J Infect Dis. 2006;194:1226–33. DOIPubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 15, Number 10—October 2009
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Frank G.J. Cobelens, Academic Medical Center, CPCD T0-126, Meibergdreef 9, 1105 AZ Amsterdam, the Netherlands
Top