Volume 15, Number 3—March 2009
Research
Capacity of Thailand to Contain an Emerging Influenza Pandemic
Cite This Article
Citation for Media
Abstract
Southeast Asia will likely be the epicenter of the next influenza pandemic. To determine whether health system resources in Thailand are sufficient to contain an emerging pandemic, we mapped health system resources in 76 provinces. We used 3 prepandemic scenarios of clustered cases and determined resource needs, availability, and gaps. We extended this analysis to a scenario of a modest pandemic and assumed that the same standards of clinical care would be required. We found that gaps exist in many resource categories, even under scenarios in which few cases occur. Such gaps are likely to be profound if a severe pandemic occurs. These gaps exist in infrastructure, personnel and materials, and surveillance capacity. Policy makers must determine whether such resource gaps can realistically be closed, ideally before a pandemic occurs. Alternatively, explicit assumptions must be made regarding allocation of scarce resources, standards of care, and priority setting during a pandemic.
The World Health Organization (WHO) has highlighted how the Asia-Pacific region has been an important center of emerging diseases such as severe acute respiratory syndrome (SARS) and avian influenza. Since 2003 (as of September 10, 2008), 15 countries have experienced human cases of infection with influenza virus A subtype H5N1 (1), and subtype H5N1 infection is now endemic in poultry in several countries. The H5N1 subtype continues to pose an important public health threat in both the short term and the long term. Southeast Asia remains a likely region from which future emerging infectious diseases, including the next influenza pandemic, are likely to emerge (2,3).
In a resolution issued in April 2005, WHO expressed concern about the general lack of global preparedness for pandemic influenza (4). Since then, considerable international efforts have been expended, and substantial resources have been committed to controlling avian influenza and preparing for pandemic influenza (5). Because the question is not whether a pandemic will occur but rather when (6), policy makers have been urged to take action in preparedness planning, including making national preparedness strategies operational (5,7,8). However, despite efforts to support preparedness, no universally accepted, organized method of evaluating preparedness exists, and concerns have been raised that implementation of many national strategic plans may be unrealistic (9,10). Several approaches have been adopted to evaluate preparedness, including assessments of national strategic plans (9,11), desk-top simulations (12), full-scale field exercises, case studies with site visits to assess health systems (8), and mathematical modeling exercises (13,14). All have particular strengths and weaknesses. Most of these approaches, although linked to national strategic and operational plans, have not included assessments of capacity to respond (that is, of available resources at each site and the potential to mobilize these resources). Without determining capacity to respond, the feasibility of effectively and efficiently implementing plans in a time of crisis remains highly uncertain.
In this article, we define and quantify, at the province level, the health system resources likely to be drawn upon in the event of WHO prepandemic phases 4 and 5 in Thailand, a relatively well-developed, middle-income, Southeast Asian country at high risk for being the epicenter of the next pandemic. We estimate gaps in resources, given several prepandemic influenza scenarios. These scenarios were previously developed by policy makers and have been used extensively in tabletop exercises in most provinces throughout the country. Our aim was to determine the challenges still remaining in preparing the country to effectively meet and contain the danger of an emergent pandemic. We addressed the challenge of mitigation in the event of a modest pandemic scenario, but, in agreement with national strategic policy, we assumed no diminution of standards of care or rationing of clinical services. Although the ability to maintain such levels of care is unlikely in reality, no national policies explicitly acknowledge this possibility; thus, this research draws on scenarios and assumptions currently guiding policy making.
Resource Mapping
The health system in Thailand is organized through 12 health regions. These regions include 76 provinces (in this article, we consider Bangkok a province). The provinces comprise 784 administrative districts; Bangkok has 50 administrative districts. We mapped the presence of resources across Thailand’s provinces. We developed a survey instrument to determine resources likely to be drawn upon at the province level if human-to-human spread of a novel influenza virus occurs. The survey instrument was developed in a stepwise manner. First, we reviewed the case notes about all human cases of avian influenza that have occurred in Thailand since 2004 and determined the resources used to manage the cases. Second, we conducted a literature review of resources used in managing influenza and SARS, and we then expanded the list of resources determined from the case notes review list. Third, we reviewed the resource list with experts in communicable disease control at national institutions and, through these discussions, modified the list.
A survey instrument was developed from the resource list and pilot tested in Kanchanaburi Province among healthcare personnel from several public health and healthcare institutions at the local, district, and province levels. Minor modifications and clarifications were made to the survey instrument as a result.
The survey instrument addressed resource needs across 4 topics of interest: surveillance, case investigation, case treatment, and prevention of spread of disease in the community. Thirty-nine resources were assessed. Data on infrastructure, personnel, and materials were collected. Province data sources were derived from the following institutional settings, which were identified through national routine health system data sources: district hospitals; subdistrict health centers; district public health offices; regional, provincial, and higher level health institutions; private healthcare facilities; and university healthcare facilities.
The survey instrument was sent to representatives of each of the 75 provinces and Bangkok in July 2007. These province representatives sent questionnaires to institutions at lower organizational levels. Duplication of data was avoided by coordinating data collection through designated institutional respondents. Those who did not respond were reminded by letter and phone calls 2 months after they had received the questionnaires.
Scenarios
Building on simulation exercises conducted in Thailand and on transmission dynamics in the published literature, we assumed 3 scenarios (14). The scenarios were previously developed by Thailand’s Department of Disease Control and made explicit assumptions about attack rates, illness, and mortality rates (15,16). As of July 2007, 66 (88%) provinces and 468 (60%) districts had conducted tabletop exercises that drew on these scenarios. Of note, these scenarios were static; that is, cases and contacts (i.e., opportunities for spread) occurred simultaneously. We assumed that the current policy focus in Thailand is on containment, rather than on mitigation. Our interest was in determining the resource gaps in WHO phases 4 and 5 (localized and substantial clusters, respectively). We did not analyze the processes of mobilizing resources or the associated logistical challenges.
Scenario 1, WHO Phase 4
This scenario assumed human-to-human transmission from case-patients to caregivers. It involved 2 patients with confirmed influenza, 3 health personnel with confirmed mild influenza, and 10 persons who were close contacts.
Scenario 2, WHO Phase 5
This scenario assumed human-to-human transmission in localized clusters. It involved 5 patients with confirmed influenza and 75 contact persons.
Scenario 3, WHO Phase 5
This scenario assumed human-to-human transmission that resulted in a substantial number of cases. One cluster of human-to-human influenza cases was identified in each of 5 districts of the province. Each cluster consisted of 5 patients with confirmed influenza (25 in total) and 375 contact persons across the province.
Resource Needs
We determined resource needs at the province level for each of the 3 above-mentioned scenarios. Resource needs were determined through retrospective analyses of case notes and discussions with clinicians and surveillance personnel intimately involved in managing earlier cases of avian influenza in persons in Thailand. For case-patients and their contacts, infrastructural, personnel, and material needs were determined. Thus, for the outbreaks, we assumed that needs were the resources used, multiplied by the number of case-patients or by the total number of contacts of the case-patients and the contacts generated respectively through different scenarios. We assumed that resource needs for any case-patient would be the same as for subsequent case-patients (that is, that resource needs are linearly related to the numbers of case-patients and their contacts as an outbreak develops).
Province Resource Gaps
We determined resource gaps at the province level for each scenario and defined influenza-specific resources. Some resources such as oseltamivir are used specifically for treatment of influenza. We assumed, therefore, that some resources were dedicated influenza resources. For oseltamivir use, we assumed that case-patients would receive treatment and that their contacts would be given prophylaxis. Other resources were nonspecific for influenza. For example, physicians would still be needed to provide essential healthcare services. We assumed, on the basis of other reports (17,18), that because resources would still be demanded by essential health services, 12% of non–influenza-dedicated resources would be available to support influenza control. That is, 88% of resources would still be dedicated to essential services. We assumed that available beds in negative-pressure rooms would be needed first, then isolation beds, then single-occupancy rooms, and so forth. We assumed that care for case-patients would be provided in hospitals and that care for contacts would be provided in the community. Some resources, such as hospital beds, cannot be shared between provinces. We assumed that other resources would not be shared between provinces in a timely manner (an unpublished qualitative analysis of the mobilization of resources showed that mobilization of resources through formal agreements is ill defined and has been difficult to achieve during simulation exercises; P. Chompook, unpub. data).
Dynamic Timeline Analysis
Although scenarios used in tabletop simulation exercises across Thailand to date have been static, in reality, WHO phases 4 and 5 are likely to emerge over several days and weeks. In a secondary analysis, we determined the needs and gaps for resources if we assumed that cases would emerge in a manner predicted by published transmission dynamics scenarios (19). We assumed that case-patients would need to be hospitalized for 7 days and that treatment with antiviral drugs would be provided to case-patients and contacts in accordance with recommendations (20).
National Resource Gaps under WHO Pandemic Phase 6
National strategic policy regarding pandemic influenza makes no explicit acknowledgment that standards of care will decrease or that allocation of scarce resources will, of necessity, demand rationing. We determined national gaps in resources under mild pandemic conditions by assuming that scenario 3 would develop evenly and simultaneously across all provinces (that is, early pandemic WHO phase 6). We first assumed perfect mobilization of resources such that provinces with excess resource capacity effectively and efficiently supported provinces with gaps. Resource gaps described under this scenario were determined by the summation of surplus and gaps in resources from all provinces. Also, under the same WHO phase 6 scenario, we assumed inadequate (imperfect) mobilization of resources across provincial borders such that resources remained within provinces. Resource gaps under this scenario were derived from the summation of gaps only from provinces where estimated resource shortfalls occur.
Data were collected from respondents at the region, province, and district levels. Data from 73 (96%) provinces were made available through respondents in 765 districts (765/834, 92%). Full data from all province institutions were provided from 53 (70%) provinces. Data from Bangkok were provided solely by public hospitals.
To determine total availability of provincial and national resources and account for missing data, we estimated the resource availability in districts where data were unavailable and extrapolated these estimations. We assumed that districts with similar numbers of hospital beds would have the same quantity of other resources available. The Ministry of Health determines bed quotas, and data were derived from routine data sources.
The average quantity of province resources is listed in the Table 1. The estimated average province resources are the result of extrapolation and correction when data points were missing. Because few data points were missing, the estimates were very similar to the averages derived from hard data. The estimated resources were further analyzed to determine resource gaps. Substantial differences in resource availability exist across provinces. We found no correlation of resources with gross provincial product (a measure of a province’s economic well-being) or with province poultry density. We found, however, correlations between some resources (for example, healthcare personnel, hospital beds, and ventilator equipment) and both population size and density (Table 1).
Figure 1

Figure 1. Density of selected health system resources available for pandemic influenza across provinces, Thailand. A) Surveillance and rapid response team personnel; B) internal medicine physicians; C) critical care nurses.
Figure 2

Figure 2. Density of selected health system resources available for pandemic influenza across provinces, Thailand. A) Negative-pressure rooms; B) adult respirators; C) surgical masks; D) oseltamivir tablets.
The differences in resource availability across provinces are illustrated through 7 selected resources (Figures 1, 2). These selected resources offer insights into the geographic variations in preparedness in relation to surveillance capacity (surveillance and rapid response team [SRRT] personnel), case investigation capacity (SRRT, internal medicine doctors), case-patient treatment capacity (oseltamivir treatment courses, respirators, critical care nurses), and capacity to prevent spread of disease in the community (negative-pressure rooms, isolation rooms, surgical masks).
Figure 3

Figure 3. Gaps in health system resources (internal medicine physicians) likely to occur for 3 scenarios of prepandemic influenza across provinces, Thailand. A) Scenario 1; B) scenario 2; C) scenario 3.
Figure 5

Figure 5. Gaps in health system resources (oseltamivir tablets) likely to occur for 3 scenarios of prepandemic influenza across provinces, Thailand. A) Scenario 1; B) scenario 2; C) scenario 3.
Gaps in resources existed in some provinces under scenario 1 (and thus for subsequent scenarios). These resource gaps include infrastructure, personnel, and materials and potentially limit capacity in all 4 control areas (surveillance capacity, case-investigation capacity, case-treatment capacity, and capacity to prevent spread of disease in the community) (Technical Appendix ). If care for case-patients is limited to negative-pressure rooms or isolation beds, then bed availability is likely to be problematic, even with a small numbers of cases. However, if beds dedicated to wider use are made available, then shortfalls are unlikely when limited cases occur. Most resource gaps are linked to critical care and include lack of trained personnel and respirators. For example, by scenario 3, 92% of provinces will have insufficient negative-pressure rooms to respond effectively to case-patients, and a severe shortage of critical care nurses will occur. However, if isolation beds are used, the proportion of provinces with insufficient resources falls to ≈75%, and if single occupancy rooms are also used, bed capacity across the country is sufficient. As the number of case-patients and contacts increases through scenarios 2 and 3, the number of provinces with gaps in resources grows. The geographic distribution of resource gaps varies, depending on resource and scenario (Figure 3–Figure 5).
Figure 6
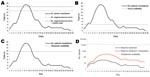
Figure 6. Projected demand and gaps in selected health system resources in Thailand, assuming prepandemic containment. A) Hospital beds; B) critical care nurses; C) adult respirators; D) oseltamivir tablets.
The need for 4 selected resources changed over time, assuming the epidemic curve (Figure 6). The gap in available resources was limited to only a few days for respiratory support. For beds, likewise, when small numbers of cases occur and case-patients are cared for in negative-pressure rooms or isolation rooms, shortages are likely to arise for only a few days. Sufficient stocks of oseltamivir are currently held at the provincial level to meet the needs of a few case-patients and their contacts.
Resource gaps exist on the national level if scenario 3 occurs simultaneously in all provinces across Thailand (Table 2). Such an event represents WHO phase 6, that is, sustained human-to-human transmission, albeit on a relatively small scale. Despite this small scale, national resource gaps are substantial if the same standard of clinical care is maintained when fewer cases arise. For some critical resources, such as internal medicine physicians and oseltamivir tablets, the problem is mitigated if we assume perfectly effective, timely, and efficient movement of resources from provinces with surplus capacity to provinces with gaps. Some resources, however, are limited in number (such as critical care nurses), and even effective redistribution may make little difference in outcome.
We showed that Thailand is likely to have some resource gaps in responding to clusters of cases in an emergent influenza pandemic and that these gaps vary across different provinces. These gaps are, however, likely to occur over a limited duration if the cases occur over several weeks and the numbers of cases are limited. As the number of cases increases, however, provincial and national capacity is likely to be tested in certain ways if clinical care and surveillance are expected to remain at a similar standard as when cases are limited. The results of such a scenario are similar for some countries of western Europe (21). Although policy makers will, in all likelihood, need to consider issues of rationing and priority setting explicitly in national strategic planning, resources in Thailand are substantial overall, although geographic distribution likely poses logistical challenges. In the event of a modest outbreak of pandemic influenza (WHO phase 6) similar to these locally developed scenarios, Thailand, a relatively affluent country in Southeast Asia, might encounter relatively modest gaps in available resources. However, if a pandemic is substantial in terms of the severity of illness and proportion of deaths, resources are likely to be insufficient, and policy makers will have to consider whether such resource gaps can be closed in reality. This conclusion has important policy implications and raises several questions. Should most resources and planning be focused explicitly on early containment potentially at the expense of mitigation, particularly in developing countries? How, to whom, and where should the deployment of scarce resources be planned (22)? A further issue raised is how realistic simulation exercises are and whether they effectively inform preparedness planning. Investment to address gaps in resources can be focused where the most important gaps exist. Some gaps, however, for example, in clinical and nursing staff, will take time and considerable investment to fill. We show at the province level where resource gaps are most profound and thus where future investment might be focused.
The variations of resources correlate strongly with both the population size and the population density of a province. Historically, healthcare resources have been distributed on the basis of provincial population size and not according to poverty indices. To date, risk assessments related to pandemic influenza have not informed planning and deployment of resources. This circumstance has potentially important implications for future preparedness planning. Provinces with relatively less dense populations, in which communication facilities are stretched to their limit and access to services is already likely to be problematic, may be further challenged by their relatively fewer resources (23). Focused investment in resources may be needed if the response to an emergent pandemic is to be equitable. Variations exist also among provinces in their resource capacity for surveillance, case investigation, case-patient treatment, and control of community spread.
Responding effectively and in a timely manner to gaps we have highlighted will be a managerial challenge. Moreover, using available resources most effectively and efficiently on a national scale also demands considerable managerial and administrative capacity (issues we did not examine). The timely mobilization of most resources remains to be planned.
This study has several limitations. First, our survey focused on the narrow clinical response and ignored the capacity of management, administrative systems, financial systems, and communications, capacities that are likely to be needed to efficiently mobilize resources (24). Second, we assumed that the relationship between resource need and case-patients is linear, and we estimated gaps on the basis of assumptions that care for case-patients as the pandemic unfolds will draw upon similarly characterized resources as in earlier phases. This assumed relationship is unlikely to occur, and care for case-patients is likely to be different from our study assumptions. However, few strategic plans explicitly acknowledge this change in resource use and thus do not plan for it (9). Third, our scenarios, although based on tabletop exercises conducted across the country, are limited in terms of anticipated case-patients and their contacts. Even though we extended our scenario to a modest pandemic, an alternative real-life scenario under which large numbers of cases occur is likely to test the health system profoundly. Fourth, we assumed that resource sharing between provinces would be limited on the basis of an analysis of formal strategic arrangements. Fifth, some data points were missing. Although the missing data were few, and corrections were possible, some of these data were from Bangkok. In Bangkok, any determination of the city’s overall resources is a challenge because of the many private autonomous healthcare facilities and their lack of systematic integration into the public health system. This factor means that our interpretation of Bangkok’s capacity to respond should be considered with caution. Bangkok has 65 private hospitals with >50 beds (14,000 beds in total), and these institutions were excluded from our survey. The challenge of coordinating the city’s resources in the event of a pandemic is substantial. Without an understanding of what and where those resources are, their management will be much more challenging. This lack of knowledge would have profound implications for Thailand because Bangkok is a city of 10 million persons, the economic powerhouse of the country, and a hub for transportation and communications with the rest of Thailand. The missing information also has important implications for the global control of a pandemic because of Bangkok’s role as a major international transport hub. If emergent pandemic influenza cannot be controlled in Bangkok, the world will be affected. The same lack of complete information would apply to other major cities where complex health systems exist.
We have shown that the health system resources available to Thailand are likely to be sufficient to respond to emergent pandemic influenza if the pandemic is modest and occurs in a manner similar to the assumptions informing Thailand’s simulation exercises. Other countries in the region, which is acknowledged to be at high risk for being at the epicenter of the next global pandemic of influenza (25), are likely to have fewer resources than Thailand (3). We are currently investigating the capacity of Thailand and neighboring countries to respond to more profound pandemic influenza scenarios. Policy makers in the region may need to reflect on where health system resources in the region might best be positioned and further expanded; what scenario assumptions are used to inform preparedness planning; whether containment, mitigation, or both, should be the focus of attention; and whether provinces with the largest probable gaps should be supported further in strengthening response capacity. Policy makers should also consider how the capacity of the private healthcare sector can, if a public health crisis occurs, be drawn upon in a timely and effective manner. In the event of a major pandemic, difficult decisions regarding the use of scarce resources will need to be made, and explicit planning ahead for the pandemic is advised.
Dr Putthasri is deputy director of the International Health Policy Programme, Ministry of Public Health, Thailand. His research interests include health systems analysis, health services research, and health economics.
Acknowledgment
This study was supported by the Rockefeller Foundation; BIOTEC (National Center for Genetic Engineering and Biotechnology); the Ministry of Science and Technology, Thailand; the London School of Hygiene and Tropical Medicine; and the Ministry of Public Health, Thailand.
References
- World Health Organization. Cumulative number of confirmed human cases of avian influenza A/(H5N1). 2008 Sep 10 [cited 2008 Sep 16]. Available from http://www.who.int/csr/disease/avian_influenza/country/cases_table_2008_09_10/en/index.html
- Russell CA, Jones TC, Barr IG, Cox NJ, Garten RJ, Gregory V, The global circulation of seasonal influenza A (H3N2) viruses. Science. 2008;320:340–6. DOIPubMedGoogle Scholar
- Jones KE, Pate NG, Levy MA, Storeygard A, Balk D, Gittleman JL, Global trends in emerging infectious diseases. Nature. 2008;451:990–3. DOIPubMedGoogle Scholar
- 58th World Health Assembly. 7 April 2005. Geneva. WHO. 2005;2005:7 [cited 2009 Jan 30]. Available from http://www.who.int/gb/e/e_wha58.html
- United Nations Systems Influenza Coordination. Responses to avian influenza and state of pandemic readiness: third global progress report. New York: The Coordination and World Bank; 2007.
- Webster RG, Govorkova EA. H5N1 influenza–continuing evolution and spread. N Engl J Med. 2006;355:2174–7. DOIPubMedGoogle Scholar
- European Centre for Disease Prevention and Control. Report for policymakers. Pandemic preparedness in the European Union, Autumn 2007. Stockholm: The Centre; 2007.
- European Centre for Disease Prevention and Control. Technical report: pandemic influenza preparedness in the EU. Status report as of Autumn 2006. Stockholm: The Centre; 2007.
- Coker R, Mounier-Jack S. Pandemic influenza preparedness in the Asia-Pacific region. Lancet. 2006;368:886–9. DOIPubMedGoogle Scholar
- Ortu G, Mounier-Jack S, Coker R. Pandemic influenza preparedness in Africa is a profound challenge for an already distressed region: analysis of national preparedness plans. Health Policy Plan. 2008;23:161–9. DOIPubMedGoogle Scholar
- Mounier-Jack S, Coker RJ. How prepared is Europe for pandemic influenza? Analysis of national plans. Lancet. 2006;367:1405–11. DOIPubMedGoogle Scholar
- World Health Organization (WHO). Exercise development guide for validating influenza pandemic preparedness plans. Manila: WHO Regional Office for the Western Pacific; 2006.
- Nap RE, Andriessen MPHM, Meesen NEL, van der Werf TS. Pandemic influenza and hospital resources. Emerg Infect Dis. 2007;13:1714–9.PubMedGoogle Scholar
- Ferguson NM, Cummings DA, Cauchemez S, Fraser C, Riley S, Meeyai A, Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature. 2005;437:209–14. DOIPubMedGoogle Scholar
- Chopitayasunondh T, Sawanpanyalert N. Clinical practice guideline for human avian influenza (H5N1). Nonthaburi (Thailand): Ministry of Public Health; 2006.
- Chunsuttiwat S, Kanchit L, Darika K, Chariya S, Naruemon S, Darin A, Table top exercises for pandemic influenza preparedness at provincial level (guideline for managers and facilitators). Nonthaburi (Thailand): Ministry of Public Health; 2006.
- Schull MJ, Stukel TA, Vermeulen MJ, Guttmann A, Zwarenstein M. Surge capacity associated with restrictions on nonurgent hospital utilization and expected admissions during an influenza pandemic: lessons from the Toronto severe acute respiratory syndrome outbreak. Acad Emerg Med. 2006;13:1228–31.PubMedGoogle Scholar
- Kanter RK, Moran JR. Hospital emergency surge capacity: an empiric New York statewide survey. Ann Emerg Med. 2007;50:314–9. DOIPubMedGoogle Scholar
- Longini IM Jr, Nizam A, Xu S, Ungchusak K, Hanshaoworakul W, Cummings DA, Containing pandemic influenza at the source. Science. 2005;309:1083–7. DOIPubMedGoogle Scholar
- Nap RE, Andriessen MP, Meessen NE, van der Werf TS. Pandemic influenza and hospital resources. Emerg Infect Dis. 2007;13:1714–9.PubMedGoogle Scholar
- World Health Organization. Ethical considerations in developing a public health response to pandemic influenza. Geneva: World Health Organization; 2007 [cited 2009 Jan 30]. Available from http://www.who.int/csr/resources/publications/WHO_CDS_EPR_GIP_2007_2c.pdf
- Wibulpolprasert S, Pengpaibon P. Integrated strategies to tackle the inequitable distribution of doctors in Thailand: four decades of experience. Hum Resour Health. 2003;1:12. DOIPubMedGoogle Scholar
- Lambrew JM, Shalala DE. Federal health policy response to Hurricane Katrina: what it was and what it could have been. JAMA. 2006;296:1394–7. DOIPubMedGoogle Scholar
- Lee VJ, Chen MI, Chan SP, Wong CS, Cutter J, Goh KT, Influenza pandemics in Singapore, a tropical, globally connected city. Emerg Infect Dis. 2007;13:1052–7.PubMedGoogle Scholar
Figures
Tables
Cite This ArticleTable of Contents – Volume 15, Number 3—March 2009
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Richard Coker, 3 Communicable Diseases Policy Research Group (CDPRG), Department of Public Health and Policy, London School of Hygiene and Tropical Medicine, Keppel St, London WC1E 7HT, UK
Top