Volume 15, Number 4—April 2009
THEME ISSUE
The Amazon Region
Dispatches
Concurrent Dengue and Malaria in Cayenne Hospital, French Guiana
Cite This Article
Citation for Media
Abstract
Dengue–malaria co-infection reports are scarce. Of 1,723 consecutive febrile patients in Cayenne Hospital, 238 had dengue (174 early dengue fever cases) and 393 had malaria (371 acute malaria); 17 had both. Diagnosis of 1 of these 2 infections should not rule out testing for the other infection.
Despite a wide overlap between malaria- and dengue-endemic areas, published reports of co-infections are scarce in the literature. The first 2 patients with concurrent malaria (Plasmodium falciparum) and dengue were identified in July 2005 (1) and November 2006 (P. vivax) (2). Since then, a few publications described proven or suspected associations, but always as isolated cases (3–6).
In French Guiana, a French territory in South America that is 92% covered by Amazon rain forest, malaria and dengue fever represent 2 major public health concerns. The annual number of P. falciparum and P. vivax malaria cases ranges from 3,500 to 4,500. In addition, all 4 dengue virus serotypes have been isolated in the country (7). To determine the frequency of concurrent infection with dengue and malaria in French Guiana, we conducted a 1-year study of patients evaluated in the emergency department of Cayenne Hospital.
Figure
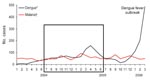
Figure. Comparison of confirmed cases of dengue fever and of symptomatic malaria in patients examined at the emergency department of Cayenne Hospital, Cayenne, French Guiana, January 2004–March 2006. The black frame corresponds to the period of the...
We carried out a retrospective study by testing blood and serum samples on 1,740 patients who consulted the emergency department of Cayenne Hospital seeking treatment for fever compatible with malaria and/or dengue during a 1-year period, July 2004–June 2005 (Figure). Diagnosis of malaria has always been quick; dengue diagnosis was initially conducted only in malaria-negative patients. In our study, dengue investigations were conducted retrospectively at the Pasteur Institute of French Guiana for 99% of patients (1,723/1,740) by using serum samples obtained at admission and frozen at –80°C. Medical records of case-patients with dengue–malaria co-infections were consulted retrospectively to look for severe or abnormal features.
Malaria diagnosis was based on the identification of hematozoa on a thin blood film and/or on a thick blood film stained with Giemsa. The screening sensitivity was ≈6 plasmodia/µL (1/1,000 leukocytes). The asexual parasite load (PL) was quantified in percent parasitized erythrocytes for values >0.1 %. For lower values, classes were created using thick smears: class 1, <0.00125% but positive; class 2, >0.00125% but <0.0125%; and class 3, >0.0125% but <0.125%. Asymptomatic Plasmodium spp. carriage was considered for classes 1 and 2 (in the absence of prior antimalarial treatment and for case-patients residing >1 year in an area of malaria transmission). Virus isolation or reverse transcription–PCR (RT-PCR) according to Lanciotti et al. (8) was performed on all serum samples obtained during the acute phase of infection, between day 0 and day 4 (n = 264). For malaria-positive samples, virus isolation was conducted on all samples without a date of onset of disease (n = 163).
Serologic immunoglobulin (Ig) M testing was performed on all serum samples (n = 1,723). Dengue was detected in 238 case-patients (13.8%); among these, 73% (174/238) were confirmed by positive virologic diagnosis (isolation or RT-PCR), whereas 27% were probable dengue cases (positive IgM serology only). The first group was named early dengue cases (EDC) and the second group late dengue cases (LDC).
Of the 1,723 patients, 393 (22.8%) had smear-positive malaria; of those, 251 (63.9%) were P. vivax, 133 (33.8%) were P. falciparum, 2 were P. malariae, and 7 were mixed P. vivax and P. falciparum. Most malaria-positive case-patients had a parasite count above class 2 (371/393 [94.4 %]), indicating acute malaria.
Concurrent dengue (EDC and LDC) and malaria were confirmed in 17 of the 1,723 patients (1%), corresponding to 7.1% (17/238) of dengue cases and 4.1% (16/393) of malaria cases, respectively (Table). When considering acute malaria associated with EDC, the percentages of confirmed associations were 3.4% for dengue (6/174, 95% confidence interval [CI] 0.7–6.2) and 1.6% for malaria (6/371, 95% CI 0.3–2.9). All 17 associations were considered clinically as malaria, including the 2 case-patients with low parasite counts. Antimalarial drugs were administered promptly in every case. Dengue serology and virology reports were available after the initial episode; however, these results did not influence patient management. Among the 6 acute concurrent infections, none was severe. The clinical evolution was always favorable. Three patients were hospitalized, all in the IgM-seropositive group, i.e., LDC; only 1 was severely ill. This patient, who had P. vivax malaria infection, was hospitalized for interstitial pneumonia with severe anemia. Intubation, blood transfusion, and antimicrobial drugs were required, but he was discharged from the intensive care unit after 11 days. No causative agent was identified for this pneumonia. The second patient was hospitalized for diabetes, the third because treatment with Riamet (arthemether + lumefantrine) was only available to inpatients.
Malaria and dengue must be suspected in febrile patients living in or returning from areas endemic for these infections. Although the usual places of contamination by malaria and dengue viruses are quite different in French Guiana, considering that the incubation phase is longer for malaria than for dengue and that the population’s mobility is high, a simultaneous clinical expression of the 2 diseases is plausible. Moreover, in French Guiana, dengue viruses have spread to malaria-endemic rural areas (9).
The confirmation of malaria is rapid, and after malaria is confirmed, dengue is usually ruled out without screening for it. Two methods can confirm dengue: dengue-specific IgM seroconversion or detection of dengue virus particles during the acute phase (day 0 to day 4 after onset of fever) by RT-PCR, which is faster and more specific. In published case reports (1–7), the diagnosis of dengue infection is usually made based on positive dengue IgM; however, this cannot confirm recent dengue, because IgM can persist for months and cross-react with other arboviruses (10). If RT-PCR requires a specific laboratory and cannot be performed on site, a new test, the Platelia, is now easily included in any laboratory and is indicated particularly for early-acute phase samples (11). To investigate the frequency of dengue and malaria co-infection, the Platelia test should be used in all cases of dengue-like or malaria-like syndrome, even when malaria diagnosis was positive, in regions where both infections may overlap.
Of the 1,723 patients investigated in this study, 17 had concurrent dengue and malaria. In 10 of these patients, recent acute dengue fever could not be confirmed (LDC). Two patients, 1 of whom was part of the EDC group, could have been asymptomatic carriers of Plasmodium spp. (1 patient with P. falciparum and 1 with P. vivax) because of low parasitemia (12). A true acute concurrent infection (strictly defined diagnosis) was confirmed in 6 case-patients. Concurrent acute malaria and recent dengue fever had a lower frequency than predicted by the multiplication of both prevalences, but such reasoning implies the same overlapping contamination areas for malaria and dengue, which it is not the situation in French Guiana. The greater prevalence of LDC than EDC associated with acute malaria infection illustrates the prolonged persistence of specific IgM or IgM cross-reaction, which increases the probability of a malaria case when comparing the short 4–5 day period corresponding to EDC. Virologic investigations using isolation or RT-PCR techniques were not performed on samples taken after the 4th day because of the usual disappearance of viremia. Additional associations where fever was initially caused by malaria and followed by dengue after the 4th day of malaria fever could have been undiagnosed.
EDC were diagnosed on average after 4 days of fever, never 5. Thus, delayed complications of dengue or malaria may not be detected using this definition. Such complications could be observed in patients considered LDC. One of these patients had pneumonia, which has recently been described as a complication of P. vivax (13).
Although acute concurrent infections were benign in our study, special attention should be given to the possibility of co-infection with malaria and dengue, especially when P. falciparum is implicated. The distinction between severe dengue and severe malaria must be made in an emergency department or hospital setting because in both situations, early diagnosis is essential for patient care.
Dr Carme is head of service in Cayenne Hospital (French Guiana) and Faculty of Medicine (French West Indies and French Guiana University), Director of Research Team EA 3593 (French Ministry of Research), and Director of Clinical Investigation Center–Clinical Epidemiology CIE 802 (Institut National de la Santé et de la Recherche Médicale). His primary interests are emerging (and reemerging) tropical parasitic diseases.
Acknowledgment
This study was supported by Cayenne Hospital, the Faculty of Medicine of French West Indies and French Guiana (EA 3593 research team), the Pasteur Institute of French Guiana, and the Clinical Investigation Centre/Clinical Epidemiology/Inserm (CIE 802) of French Guiana and French West Indies.
References
- Charrel RN, Brouqui P, Foucault C, de Lamballerie X. Concurrent dengue and malaria. Emerg Infect Dis. 2005;11:1153–4.PubMedGoogle Scholar
- Deresinski S. Concurrent Plasmodium vivax malaria and dengue. Emerg Infect Dis. 2006;12:1802.PubMedGoogle Scholar
- Thangaratham PS, Jeevan MK, Rajendran R, Samuel PP, Tyagi BK. Dual infection by dengue virus and Plasmodium vivax in Alappuzha District, Kerala, India. Jpn J Infect Dis. 2006;59:211–2.PubMedGoogle Scholar
- Bhalla A, Sharma N, Sharma A, Suri V. Concurrent infection with dengue and malaria. Indian J Med Sci. 2006;60:330–1.PubMedGoogle Scholar
- Ward DI. A case of fatal Plasmodium falciparum malaria complicated by acute dengue fever in East Timor. Am J Trop Med Hyg. 2006;75:182–5.PubMedGoogle Scholar
- Kaushik RM, Varma A, Kaushik R, Gaur KJ. Concurrent dengue and malaria due to Plasmodium falciparum and P. vivax. Trans R Soc Trop Med Hyg. 2007;101:1048–50. DOIPubMedGoogle Scholar
- Reynes JM, Laurent A, Deubel V, Telliam E, Moreau JP. The first epidemic of dengue hemorrhagic fever in French Guiana. Am J Trop Med Hyg. 1994;51:545–53.PubMedGoogle Scholar
- Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ, Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J Clin Microbiol. 1992;30:545–51.PubMedGoogle Scholar
- Tran A, Deparis X, Dusssart P, Morvan J, Rabarison P, Remy F, Dengue spatial and temporal patterns, French Guiana, 2001. Emerg Infect Dis. 2004;10:615–21.PubMedGoogle Scholar
- Allwinn R, Doerr HW, Emmerich P, Schmitz H, Preiser W. Cross-reactivity in flavivirus serology: new implications of an old finding? Med Microbiol Immunol (Berl). 2002;190:199–202.
- Dussart P, Labeau B, Lagathu G, Louis P, Nunes MR, Rodrigues SG, Evaluation of an enzyme immunoassay for detection of dengue virus NS1 antigen in human serum. Clin Vaccine Immunol. 2006;13:1185–9. DOIPubMedGoogle Scholar
- Alves FP, Durlacher RR, Menezes MJ, Krieger H, Silva LH, Camargo EP. High prevalence of asymptomatic Plasmodium vivax and Plasmodium falciparum infections in native Amazonian populations. Am J Trop Med Hyg. 2002;66:641–8.PubMedGoogle Scholar
- Price L, Planche T, Rayner C, Krishna S. Acute respiratory distress syndrome in Plasmodium vivax malaria: case report and review of the literature. Trans R Soc Trop Med Hyg. 2007;101:655–9. DOIPubMedGoogle Scholar
Figure
Table
Cite This ArticleTable of Contents – Volume 15, Number 4—April 2009
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Bernard Carme, Faculté de Médecine et Centre Hospitalier, Parasitologie et Mycologie, Rue des Flamboyants, Cayenne F-97306, French Guiana
Top