Volume 31, Number 7—July 2025
Research Letter
Genomic Deletion of PfHRP2 and PfHRP3 in Plasmodium falciparum Strains, Ethiopia, 2009
Cite This Article
Citation for Media
Abstract
Plasmodium falciparum strains lacking P. falciparum histidine-rich protein 2 (PfHRP2) and PfHRP3 threaten malaria rapid test reliability. We show that pfhrp2/pfhrp3–deleted parasites circulated in Ethiopia as early as 2009, before widespread PfHRP2-based rapid test use, and had high pfhrp3 deletion prevalence. Monitoring of pfhrp2 and of pfhrp3 deletions is needed.
Malaria caused by Plasmodium falciparum remains a major health problem. In 2023, an estimated 263 million cases and 597,000 deaths were seen worldwide; most were in Africa. Introduction of rapid diagnostic tests (RDTs) has substantially increased malaria diagnosis and malaria control. P. falciparum histidine-rich protein 2 (PfHRP2)–detecting RDTs rely on monoclonal antibodies raised against PfHRP2. Those monoclonal antibodies cross-detect PfHRP3 because of shared amino acid repeats.
The development of malaria RDTs began in the early 1990s; however, it was not until 2008 that quality-controlled and reliable RDTs became available. The World Health Organization policy shift in 2010 to a test-and-treat strategy boosted widespread use of RDTs, and RDT sales increased to >415 million in 2022 (1). In 2010 in the Amazon region of Peru, researchers identified the first P. falciparum strains that lacked the pfhrp2 gene (and pfhrp3 gene) and caused false-negative PfHRP2 RDT results (2). Subsequent studies identified pfhrp2 gene–deleted and pfhrp3 gene–deleted parasites in other malaria-endemic regions; the highest frequencies were reported in the Amazon region in South America and parts of East Africa, including Ethiopia (3). The high frequency of gene deletions in countries in East Africa has already led to a policy switch toward non-PfHRP2 RDTs in Eritrea, Djibouti, and, in 2022, Ethiopia (4), despite the lack of reliable alternative RDT types.
We suspected that treatment guided by PfHRP2-based RDTs selects for PfHRP2 test–negative parasites that can be further transmitted and spread (3). In the Amazon region of Peru, where the first pfhrp2-deleted and pfhrp3-deleted parasites were found, PfHRP2-based RDTs were not in common use (2). To shed light on the multifactorial forces driving the spread of parasites with gene deletions, we retrospectively analyzed samples collected in Ethiopia in 2009, which was a time when PfHRP2-based RDTs were not yet used globally. We obtained the samples from eastern and southwestern regions of the country (Appendix Figure 1).
Figure
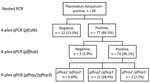
Figure. pfhrp2 and pfhrp3 deletion frequency in genomic deletion of PfHRP2 and PfHRP3 antigens in Plasmodium falciparum strains, Ethiopia, 2009. P. falciparum–positive...
We used 4-plex quantitative PCR (qPCR) analysis on 89 samples that had already tested positive for P. falciparum monoinfection by using species-specific PCR as previously reported (5) and that were available in sufficient quantities for testing (6) (Appendix); 74 were quality confirmed. Of those 74 samples, 2 (2.7%) were negative for pfhrp2 and pfhrp3 (pfhrp2−/pfhrp3−) (Figure). We did not detect any pfhrp2 single deletions (pfhrp2−/pfhrp3+), but 21 samples (28.4%) lacked pfhrp3 (pfhrp2+/pfhrp3−). Because sample size was limited, we were unable to analyze regional differences. Most (63/74) samples were from the southwestern (Jimma) region, where >90% of the deletions were found (Table). PfHRP2 RDTs were not performed on the sample set.
To further profile the pfhrp3 gene locus in the 23 samples lacking pfhrp3 (targeting the 5′ end of pfhrp3 exon 2), we reassessed the samples by using a modified 4-plex qPCR that targets the 3′ region of pfhrp3 exon 2 (7) (Appendix Figure 2). Of 21 analyzed samples (2 samples had insufficient material), 7 samples were positive for pfhrp3 (Appendix Table 1). We profiled 5 of those samples (2 samples lacked material) by PCR (primer pairs 3, 4, and 5) that spanned various regions within the pfhrp3 locus. All 5 samples had a pfhrp3 gene deletion (Appendix Table 2, Figure 2). We therefore recommend continued use of unmodified 4-plex qPCR (6).
Studies of pfhrp2 and pfhrp3 deletions in the P. falciparum population in Africa with a sufficiently large sample size are lacking (8). Before intensive use of PfHRP2-based RDTs, parasites with pfhrp2 deletions were already present but at very low frequencies and only in association with pfhrp3 deletions. In contrast, the percentage (28%) of pfhrp3-deleted parasites was surprisingly high and agrees with multiple studies from Ethiopia conducted since 2015 (Appendix Table 3).
Our data clarify the emergence and spread of PfHRP2 diagnostic–resistant parasites, supporting Feleke et al. (3). Frequently occurring pfhrp3 deletions might favor selection and spread of occasionally occurring pfhrp2 deletions under the selective pressure of intensive use of PfHRP2 RDTs followed by antimalarial treatment. Studies published in 2020 and 2021 identified a major role of PfHRP3 in the accuracy of PfHRP2 RDTs, particularly at low parasitemia, where cross-binding can mask pfhrp2 deletions and result in a positive test (9,10). In contrast, absence of PfHRP3 in pfhrp2-deleted strains results in a false-negative RDT and ultimately leads to positive selection of pfhrp2-deleted P. falciparum. Those results are particularly relevant in areas of low transmission and with extensive use of PfHRP2 RDTs and antimalarial treatment (3; O.J. Watson et al., unpub. data, http://medrxiv.org/lookup/doi/10.1101/2023.10.21.23297352). The frequency of pfhrp2 and pfhrp3 deletions is much lower in West and Central Africa countries that have a high transmission rate (O.J. Watson et al., unpub. data).
Use of different molecular tests provided valuable insights into the challenges of deletion detection and nature of pfhrp3 gene deletion. We confirmed 4-plex qPCR results by using 3 PCRs with commonly used primers and highlight that outcomes might vary depending on the assays applied. pfhrp3 deletions might contribute to the spread of pfhrp2-deleted P. falciparum and should be routinely monitored along with pfhrp2 in deletion surveillance studies.
Dr. Woldearegai is a postdoctoral researcher at the Institute of Tropical Medicine, University Hospital Tübingen, Tübingen, Germany. His primary research interests include diagnostics, molecular epidemiology, and transmission of malaria and other tropical infectious diseases.
References
- World Health Organization. T3: test, treat and track: scaling up diagnostic testing, treatment and surveillance for malaria. Geneva: The Organization; 2012.
- Gamboa D, Ho MF, Bendezu J, Torres K, Chiodini PL, Barnwell JW, et al. A large proportion of P. falciparum isolates in the Amazon region of Peru lack pfhrp2 and pfhrp3: implications for malaria rapid diagnostic tests. PLoS One. 2010;5:
e8091 . DOIPubMedGoogle Scholar - Feleke SM, Reichert EN, Mohammed H, Brhane BG, Mekete K, Mamo H, et al. Plasmodium falciparum is evolving to escape malaria rapid diagnostic tests in Ethiopia. Nat Microbiol. 2021;6:1289–99. DOIPubMedGoogle Scholar
- Federal Democratic Republic of Ethiopia, Ministry of Health. National malaria guidelines, 5th edition [cited 2025 Feb 24]. https://www.scribd.com/document/589612562/National-Malaria-Guideline-2022
- Woldearegai TG, Kremsner PG, Kun JFJ, Mordmüller B. Plasmodium vivax malaria in Duffy-negative individuals from Ethiopia. Trans R Soc Trop Med Hyg. 2013;107:328–31. DOIPubMedGoogle Scholar
- Krueger T, Ikegbunam M, Lissom A, Sandri TL, Ntabi JDM, Djontu JC, et al. Low prevalence of Plasmodium falciparum histidine-rich protein 2 and 3 gene deletions—a multiregional study in Central and West Africa. Pathogens. 2023;12:455. DOIPubMedGoogle Scholar
- Grignard L, Nolder D, Sepulveda N, Berhane A, Mihreteab S, Kaaya R, et al. Corrigendum to ‘A novel multiplex qPCR assay for detection of Plasmodium falciparum with histidine-rich protein 2 and 3 (pfhrp2 and pfhrp3) deletions in polyclonal infections’. EBioMedicine. 2021;65:
103261 . DOIPubMedGoogle Scholar - World Health Organization. Malaria threat map [cited 2024 May 7]. https://apps.who.int/malaria/maps/threats/#/maps?theme=diagnosis&mapType=diagnosis%3A0&bounds=%5B%5B-204.77944076891063%2C-57.16726526146551%5D%2C%5B204.77944076891237%2C77.99489257835737%5D%5D&insecticideClass=PYRETHROIDS&insecticideTypes=&assayTypes=&synergistTypes=&species=&vectorSpecies=&surveyTypes=&plasmodiumSpecies=&drugs=&mmType=1&excludeLowerPatients=false&excludeLowerSamples=false&endemicity=false&storyMode=false&storyModeStep=0&years=1996%2C2009&deletionType=HRP2_HRP3_PROPORTION_DELETION
- Gatton ML, Chaudhry A, Glenn J, Wilson S, Ah Y, Kong A, et al. Impact of Plasmodium falciparum gene deletions on malaria rapid diagnostic test performance. Malar J. 2020;19:392. DOIPubMedGoogle Scholar
- Kong A, Wilson SA, Ah Y, Nace D, Rogier E, Aidoo M. HRP2 and HRP3 cross-reactivity and implications for HRP2-based RDT use in regions with Plasmodium falciparum hrp2 gene deletions. Malar J. 2021;20:207. DOIPubMedGoogle Scholar
Figure
Table
Cite This ArticleOriginal Publication Date: May 28, 2025
Table of Contents – Volume 31, Number 7—July 2025
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Andrea Kreidenweiss, Institute of Tropical Medicine, University Hospital Tübingen, Wilhelmstrasse 27, D-72074 Tübingen, Germany
Top