Volume 27, Number 2—February 2021
Research Letter
COVID-19 and Infant Hospitalizations for Seasonal Respiratory Virus Infections, New Zealand, 2020
Cite This Article
Citation for Media
Abstract
In March 2020, a national elimination strategy for coronavirus disease was introduced in New Zealand. Since then, hospitalizations for lower respiratory tract infection among infants <2 years of age and cases of respiratory syncytial or influenza virus infection have dramatically decreased. These findings indicate additional benefits of coronavirus disease control strategies.
In New Zealand, the incidence of hospitalization of infants with lower respiratory tract infection (LRTI) is high. LRTIs disproportionately affect Māori and Pacific Islander children and are predominantly caused by respiratory syncytial virus (RSV) (1).
The first case of coronavirus disease (COVID-19) in New Zealand was identified on February 28, 2020. Subsequently, the government pursued an elimination strategy, commencing with a national lockdown on March 25, along with strict international border controls, mandatory 14-day isolation of all international arriving passengers, intensive community testing, school closures, and contact tracing. This strategy seems to have largely succeeded, although recent small clusters of cases in the Auckland region demonstrate continuing vulnerabilities (2).
Kidz First Children’s Hospital serves an urban population of ≈550,000 persons in South Auckland, where 50% of infants are of Māori or Pacific Islander ethnicity. Since 2007, clinicians have performed nasopharyngeal sampling for respiratory virus PCR when clinically indicated and have participated in the SHIVERS (Southern Hemisphere Influenza Vaccine Effectiveness Surveillance) program of multiplex PCR virus surveillance (2). Since March 2020, additional COVID-19 PCR testing has been routinely performed for hospitalized children with respiratory illness. Influenza vaccine, although recommended for pregnant women and high-risk infants and children, is not routinely administered. During winter–spring 2019, a large measles outbreak occurred in Auckland and hospitalizations increased. From 2016 through 2019, a randomized clinical trial of RSV vaccine for pregnant women was conducted with 152 South Auckland mother–infant pairs (3).
After COVID-19 lockdown measures were implemented, we observed a marked reduction in hospitalizations of infants for respiratory illness at Kidz First Hospital; the reduction was sustained after gradual easing of the national lockdown beginning on April 27, 2020. To confirm the decrease, we examined respiratory viral PCR test results and infant LRTI hospitalization data from January 1, 2015, through August 31, 2020. We reviewed clinical and laboratory records of infants <2 years of age hospitalized for >3 hours during that time for LRTI (codes J22, A37, J47, J10.0 J10.1 J11.1, J12–16, J20, J21, and J18 from the International Classification of Diseases, 10th Revision). All specimens submitted by a clinician for respiratory viral PCR testing were identified. Re-admissions and duplicate tests were not excluded from this dataset.
Figure
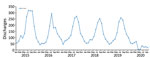
Figure. Hospital discharges among children <2 years of age with lower respiratory tract infection, South Auckland, New Zealand, 2015–2019.
Annual numbers of hospitalizations for LRTI during 2015–2019 varied from 1,486 to 2,046. A characteristic winter peak in hospitalizations occurred during July and August; however, from January 1 through August 31, 2020, only 268 admissions were reported, with no winter peak observed (Figure). Numbers of clinician-directed PCR tests performed during March 1–August 31 during the 6-year study period are similar except for increased testing in 2019 during the major measles outbreak (Table). Since March 2020, the numbers of hospitalizations associated with a positive PCR result for RSV (n = 2) and influenza (n = 1) have plummeted; however, hospitalizations for adenovirus and rhinovirus/enterovirus (positive by PCR) have persisted at levels similar to previous years. No hospitalized children have received positive COVID-19 test results.
The New Zealand COVID-19 elimination strategy seems to have halted transmission of seasonal RSV and influenza virus to infants in South Auckland; similar findings have been reported for other populations around the world, focused mainly on influenza reductions (4–8). The most likely influence on the virtual absence of RSV and influenza disease affecting infants (during what would usually be the peak winter season in New Zealand) is international border controls, including mandatory 14-day isolation of arriving passengers, limiting seasonal virus ingress to the country, although physical distancing and hygiene measures undoubtedly play a part. This hypothesis is further supported by the persistence of rhinovirus/enterovirus infections and lack of rebound of RSV and influenza infections when lockdown measures were gradually eased from late April on. The persistence of disease burdens from viruses that circulate all year suggests that although border controls have prevented entry of the seasonal viruses into the population, community preventive measures have had a more limited effect on the transmission of regional endemic viruses that cause infant hospitalizations.
Our findings are supported by the informative comparison of data across 6 years, during which time the clinician-directed investigation of infants with respiratory infections has remained consistent. Although these preliminary single-center findings need confirmation over a complete year and with national-level surveillance data, they closely align with emerging reports from Alaska, Australia, and Finland (5,8,9).
The current global situation emphasizes the need for ongoing comprehensive respiratory virus surveillance in vulnerable populations, as demonstrated by the unexpected benefit seen locally for Māori and Pacific Islander infants. As the Northern Hemisphere winter approaches, the population-level benefits of substantially reduced RSV and influenza burden may usefully inform policy makers about the merits of different COVID-19 control strategies (10).
Dr. Trenholme is a pediatrician at Kidz First Hospital, South Auckland, and a clinician–researcher with a research interest in pediatric respiratory diseases, especially bronchiectasis, influenza, and RSV.
Acknowledgments
We acknowledge the Māori and Pacific Islander children of South Auckland and their families who bear an inequitable burden of childhood respiratory disease. We thank the SHIVERS team, particularly Sue Huang and Namrata Prasad, who have contributed to improved understanding of the local pediatric RSV disease burden. We thank colleagues Emma Best, Susan Morpeth, and Conroy Wong for their support. Drs. Wong and Prasad also provided helpful review of the manuscript.
A.T. and S.L. received funding from Novavax and Medimmune corporations during the conduct of the study. R.W. received grants from the Starship Foundation and University of Auckland. C.A.B. received grants from CureKids, the Health Research Council of New Zealand, Auckland Medical Research Foundation, and National Health and Medical and Health Research Council of Australia. S.A. received grants from the Health Research Council of New Zealand.
References
- Prasad N, Trenholme AA, Huang QS, Duque J, Grant CC, Newbern EC. Respiratory virus-related emergency department visits and hospitalizations among infants in New Zealand. Pediatr Infect Dis J. 2020;39:e176–82. DOIPubMedGoogle Scholar
- Baker MG, Wilson N, Anglemyer A. Successful elimination of Covid-19 transmission in New Zealand. N Engl J Med. 2020;383:
e56 . DOIPubMedGoogle Scholar - Madhi SA, Polack FP, Piedra PA, Munoz FM, Trenholme AA, Simões EAF, et al.; Prepare Study Group. Respiratory syncytial virus vaccination during pregnancy and effects in infants. N Engl J Med. 2020;383:426–39. DOIPubMedGoogle Scholar
- Iacobucci G. Covid lockdown: England sees fewer cases of colds, flu, and bronchitis. BMJ. 2020;370:m3182. DOIPubMedGoogle Scholar
- Kuitunen I, Artama M, Mäkelä L, Backman K, Heiskanen-Kosma T, Renko M. Effect of social distancing due to the COVID-19 pandemic on the incidence of viral respiratory tract infections in children in Finland during Early 2020. Pediatr Infect Dis J. 2020;39:e423–7.PubMedGoogle Scholar
- Itaya T, Furuse Y, Jindai K. Does COVID-19 infection impact on the trend of seasonal influenza infection? 11 countries and regions, from 2014 to 2020. Int J Infect Dis. 2020;97:78–80. DOIPubMedGoogle Scholar
- Soo RJJ, Chiew CJ, Ma S, Pung R, Lee V. Decreased influenza incidence under COVID-19 control measures, Singapore. Emerg Infect Dis. 2020;26:1933–5. DOIPubMedGoogle Scholar
- Nolen LD, Seeman S, Bruden D, Klejka J, Desnoyers C, Tiesinga J, et al. Impact of social distancing and travel restrictions on non-COVID-19 respiratory hospital admissions in young children in rural Alaska. Clin Infect Dis. 2020;
ciaa1328 ; Epub ahead of print. DOIPubMedGoogle Scholar - Britton PN, Hu N, Saravanos G, Shrapnel J, Davis J, Snelling T, et al. COVID-19 public health measures and respiratory syncytial virus. Lancet Child Adolesc Health. 2020;4:e42–3. DOIPubMedGoogle Scholar
- Solomon DA, Sherman AC, Kanjilal S. Influenza in the COVID-19 Era. JAMA. 2020;324:1342–3. DOIPubMedGoogle Scholar
Figure
Table
Cite This ArticleOriginal Publication Date: December 02, 2020
1These first authors contributed equally to this article.
Table of Contents – Volume 27, Number 2—February 2021
| EID Search Options |
|---|
|
|
|
|
|
|
Please use the form below to submit correspondence to the authors or contact them at the following address:
Adrian Trenholme, Kidz First, Middlemore Hospital, Private Bag 93311, Auckland 1640, New Zealand
Top